Psychosis can happen to anyone and affects up to 3 in 100 young people in Scotland. Up to 10 per cent of people will at some point in their life hear a voice talking to them when there is no-one there. Many people who have these kinds of experiences do not come into contact with mental health services because they do not find their experiences distressing. Some people, however, are very distressed and find it difficult to cope so they seek professional help, or others seek help on their behalf.
People who seek help with psychotic experiences are sometimes given a diagnosis of schizophrenia or bipolar disorder. Psychosis can also be linked to very severe depression. There are a number of things which seem to be linked to psychosis or to make the symptoms worse. These include:
- Alcohol and drugs, especially street drugs like cannabis, speed (amphetamines) and cocaine. New synthetic drugs (so-called “legal highs”) can cause severe psychotic symptoms
- Other health problems, like head injury or epilepsy
- Severe, prolonged stress or trauma
- Severe social problems such as poverty, isolation or lots of stressors such as poor housing, overwork or relationship difficulties.
It is not clear what causes psychosis but it is probably a complex interaction between life circumstances, the way we see the world and our biological make-up.
There is sometimes confusion about what psychosis means. Psychosis has nothing to do with the terms “psycho”, or “psychopath”. It is very rare for people with a diagnosis of psychosis to be violent to others.
Many people have had one or two brief “psychotic” experiences, and they are not always a cause for concern. But it’s important to speak to your GP about this because some kinds of psychosis need treatment.
Getting help early helps people to make a better recovery.
People with psychosis can’t always recognise what’s happening to them: they might think there’s nothing wrong, and be reluctant to visit their GP. It’s important that family and friends try to persuade them to get help. If that’s not possible, you should consider getting confidential advice from their GP.
More information about psychosis is available from See Me and NHS Choices.
Acknowledgement:
Understanding Psychosis and Schizophrenia (2017) © British Psychological Society licensed under Creative Commons (CC BY-NC-ND)
More Information
What helps
You should see your GP straight away if you are having psychotic experiences. Early treatment of psychosis gives the best chance of recovery.
NHS Choices has some useful information about the kinds of question your GP may ask about psychosis. If they think your psychotic experiences might be caused by mental illness, they will arrange for you to be seen promptly by a specialist.
For people who live in the NHS Greater Glasgow and Clyde area, that is likely to be the “Esteem” team, a service for people with a first episode of psychosis. The team has bases throughout the Greater Glasgow and Clyde area.
Other people may be seen by a Community Mental Health Team (CMHT) in their local area. CMHTs can offer help from the following healthcare professionals:
- A psychiatrist – a qualified medical doctor who has received further training in treating mental health conditions
- A psychologist – a healthcare professional who specialises in the treatment of mental health conditions through talking therapies
- A community mental health nurse – a nurse with specialist training in mental health conditions
The main treatments for psychosis include:
- Medicines – Most people find that antipsychotic medicines (such as risperidone, olanzapine and clozapine) are very helpful. They can reduce or stop hallucinations and help people to think clearly again. They usually take a week or more to start working, and many people take them long-term. However they do have side effects, and it may take some time to find the right drug for you.
- Psychological treatment Cognitive Behavioural Therapy (CBT) for psychosis can be an effective way to tackle unhelpful thoughts and feelings that might be caused by psychosis.
- Family support Behavioural Family Therapy (BFT) is a useful way to help you and your family cope with psychosis, while minimising the stress of living with that condition. It should be available in your area if you live in Greater Glasgow and Clyde.
- Peer support – It’s often helpful to link up with others who have had a similar experience of illness to you. Support in Mind Scotland have particular experience of psychosis. You might also contact the Mental Health Network if you live in Glasgow, or Acumen if you live in Renfrewshire, East Renfrewshire, West Dunbartonshire or Inverclyde.
Find out more about treatments at NHS Choices.
Some people become so ill with psychosis that they’re temporarily unable to make good decisions about their care. If that happens, and there’s a risk to the health and safety of that person or to others, then doctors can use the Mental Health Act in Scotland to ensure people have the right care and treatment. Long-term decisions about care and treatment are made by the Mental Health Tribunal for Scotland, and the Mental Welfare Commission for Scotland works to ensure that peoples’ rights are respected.
Living with…Psychosis
Many people who hear voices or see visions are not troubled by them and do not seek help. For those who do, around half will completely recover after just one occasion. Some people do experience on-going difficulties. When we feel stressed or anxious, the way we think about ourselves, other people and the world around us can change. For example, we may become more self critical or fearful. There are close links between emotional distress and psychosis. Anything we can do to help with emotional problems is therefore also likely to help with symptoms of psychosis. Below are some ideas about ways to manage difficult emotions and stress.
Looking After Yourself
Taking time to look after yourself is an important part of recovery.
Think about:
- Eating regularly
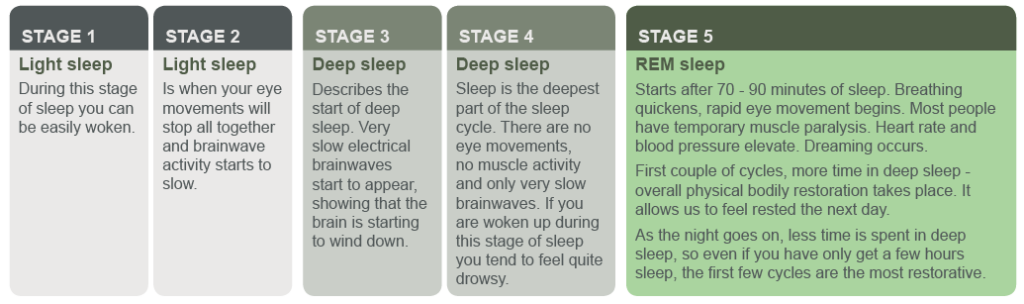
- Getting enough sleep
- Getting some exercise. Exercise is good for mental health as well as physical health. Try to get 30 minutes a day of moderate exercise if you can. NHS Choices has some good suggestions to get started if you’re not used to exercising
- Some people find mindfulness or yoga especially helpful. Although not always available through the NHS, there should be classes in your area
- Keeping in touch with people who make you feel good about yourself
- Avoiding too much alcohol or caffeine, including energy drinks
- Avoiding non-prescription drugs. Cannabis, speed (amphetamines), ecstasy, cocaine, mushrooms and so-called “legal highs” can all make your symptoms worse.
Find a Routine
Everyone needs a reason to get up in the morning so set your alarm. Plan one activity you enjoy and one which gives you satisfaction every day. Try to stick to your plan even if you don’t feel like it at times.
Write down all the things you like doing and people you like to see, and come up with a plan to start doing things and seeing people at your own pace.
If you build up to things at your own pace, over time you’ll be able to do more and more. Your family, friends or your mental health worker can help you make a plan for this.
It may be helpful to keep a diary, recording life events, your mood, your diet and sleep. This can help you recognise patterns in your moods and psychosis, and identify what might trigger it or make it worse. It can also help you identify things that have been helpful, and recognise warning signs that tell you when you are starting to feel worse.
Getting appropriate help
Stay in touch. Make sure that trusted family and friends know how you’re really feeling. It’s important to discuss symptoms, side effects and any other concerns with the clinicians working with you.
Watch out for low mood. Many people experience low mood or depression, either as part of their psychosis or as they recover from psychosis and get back to their usual lives. Let your psychologist, doctor or nurse know about this – they should be able to help. Suicidal thoughts at times are also common, and it’s especially important that you let someone know if that is troubling you.
Since some medicines taken to control psychosis can make you gain weight, it’s really important to know your weight (and BMI), and to eat healthily. Since medicines and weight gain might increase your risk of diabetes or high cholesterol, make sure these are checked by your doctor.
If you are a smoker, do all you can to quit. Stopping smoking will improve your mental health as well as your physical health. The Smokeline service might be able to help.
Managing Symptoms
There are lots of helpful things you can do to help you deal with distressing symptoms. Everyone’s experiences of psychosis are different so not all of these ideas may be useful to you. You could try out some of these ideas as other people have found them helpful.
Hearing Voices
Distraction
Some people are able to get control over their voices by distracting themselves by:
- Humming
- Listening to music
- Talking to or contacting a friend
- Playing computer games or using your phone
- Doing everyday things around the house
- Seeing friends.
Responding to Voices
- Sometimes if you talk to the voices, they will go away. You can talk into your phone when speaking to the voices to avoid bringing attention to yourself
- Imagine turning down the volume on the voices, like you would on the TV
- Keep a note of when the voices speak to you and what they say to see if these things are important to you.
Upsetting Ideas or Beliefs
Keep calm
Even though you may think or feel something is real, it may not be. Very often things we believe strongly can turn out to be wrong, so try to remind yourself of this. Try to work out what is different about times when the belief does not feel so strong and write down what you notice.
Keep busy
When you’re busy playing a sport, doing a bit of work, doing the shopping or hanging out with friends, the ideas can feel less upsetting or important.
Keep safe
Try not to act on your beliefs even if you have a very strong urge to, as this can keep your worries going. Talk to someone you trust – a family member, a friend, mental health worker or psychologist. Be aware that simple things like crossing the road can become difficult when you are very distracted.
Looking after someone with…Psychotic symptoms
As a friend, family member or partner, you can have an important role in supporting your loved one. You can help them learn to manage their psychosis and reduce the likelihood of them becoming unwell.
However, it can be difficult to know how best to help. Below are some suggestions that might be useful to you.
Helping with Unusual Experiences
Hearing voices is often very distressing for someone, as the voices are often critical and say unpleasant things. Some people may wish to talk about what the voices are saying, while others prefer to keep this private.
If the person wishes to speak about their voices, try to understand how they feel, even if you may not agree with their explanation of the voices. You can also try to point out the person’s good points to boost their confidence, as the voices will often try to undermine this.
It can help to distract the person by starting conversations or getting them involved in day-to-day activities. You could also ask the person what works for them as they may have found other ways to cope with the voices.
When people have unusual ideas or beliefs, it can be difficult to understand where these come from. It is often tempting to try to talk them out of their beliefs but this can sometimes lead to heated conversations.
Try to keep calm, even if the person is saying things that seem very frightening, and reassure them by showing them you understand how significant their beliefs are to them.
Helping with Problems with Motivation
Psychosis can make it hard for a person to:
- Think straight
- Keep going
- Take an interest in people
- Keep up with things they previously enjoyed.
While this can be frustrating for those trying supporting them, try not to expect the person to do too much too soon. It is important to strike the balance between gentle encouragement and making allowances for their difficulties. Offer praise for any achievement, however small, and try to find enjoyable or practical things to do together.
What Else Can Help?
Help the person to regain their confidence by encouraging them to do things on their own.
As it can be hard for the person to realise that others in the family may also need support or help, give clear, calm messages about what you would like to happen.
Stick to an everyday routine with regular mealtimes and chores.
Like everyone, the person may need their own time and space, so try to respect this without worrying too much.
As the person can sometimes seem distant or unemotional, show support and acceptance by continuing to spend time with them and involving them in everyday things.
Getting help
Someone who is experiencing a psychotic episode might not be aware of the changes in their thinking and behaviour. It might often fall to friends or family member to support individuals in accessing help. If someone you know needs help urgently, you have two options:
- Make an urgent appointment with their GP
- Call NHS 24 by dialling 111
How services can help family and friends to support people
Many families find it helpful to meet with a professional who is trained in helping families. The aims of these meetings could include: developing a shared understanding of what is happening, improving family relationships, and finding ways to solve problems together. Guidelines recommend that everyone diagnosed with psychosis can access family interventions. These should be available in your area if you live in Greater Glasgow and Clyde.
Even if the person does not want personal information shared with relatives, services can give you general information about the problems people experience, what can help, and what support is available.
While it is important for staff to keep information about the person’s care private, sometimes the people who live with the person or know them well may have ideas or information, which can help in their care. It is fine to pass this information on to staff if you think it might help.
Look After Yourself
Seeing someone you care about experiencing psychosis can be distressing and confusing. It is important to take care of yourself.
It can be difficult to support your relative and look after yourself at the same time. However, it is very important to make time for yourself to ensure that you do not become overwhelmed by what is happening to the person you care about.
This might mean taking time out for yourself and doing the things that are important to you, like seeing friends or keeping up with your interests. Keeping to the same routines in your day-to-day life can also reduce tension at home.
You may also find speaking to others in a similar situation useful.
Below are some resources you may find helpful:
- Support in Mind
- GAMH Carers Support
- Carers Link East Dunbartonshire
- Carers of West Dunbartonshire
- East Renfrewshire Carers Centre
- Renfrewshire Carers Centre
- Inverclyde Carers Centre
Further information for carers is available on the NHS Greater Glasgow and Clyde carers site
Early Intervention
Early treatment of a psychosis gives the best chance of recovery.
An early intervention programme, of up to 2 years, is recommended for people aged 16-35 who appear to be experiencing a first episode of psychosis.
Early interventions, for people who experience a first episode psychosis, are known to positively impact on engagement with mental health services, access to family & other psychological interventions and on future education & employment prospects and social & functional recovery.
Early intervention programmes offer different types of support that have been shown to help people recover from psychosis, and usually include practical support, family work, psychological therapy and medication. There would also be a focus on minimalising the effect of psychosis such as feelings of loss, entrapment and humiliation.
What are the potential long-term problems of untreated psychosis?
The risks include suicide, more likely to relapse, greater resistance to treatment, higher incidence of requiring compulsory care, poorer engagement with treatment, higher rates of substance miss-use, and greater distress amongst family members
“The course of schizophrenia is most stormy at onset and early in its manifest course, plateauing thereafter”
The plateau effect and the critical phase (Birchwood et al, 1998)
What could you expect from an early intervention programme?
There would commonly be a range of support/interventions available, nurses or occupational therapists would help you think about what might be most useful to you, psychiatrists would talk to you about medication options, a clinical psychologist can help with talking therapy, whilst a support worker could help you to get you out and about more.
What about hospital?
Early interventions may sometimes require a short stay in hospital, especially if you are very distressed by their experiences. There could also be some crisis or assertive outreach interventions.
What can early intervention work help with?
Early intervention work will focus on:
- Helping you try to understand the things that led to your experiences of psychosis
- Exploring ways to help with your recovery
- Working with your family and friends to encourage positive relationships
- Offering practical support with things like housing or finances
- Supporting you to return to work, university or college, or identifying ways to spend your time
Early interventions also means working with your family and friends by:
- Involving them in all aspects of your care, if you feel this would be helpful
- Offering group sessions for support
- Offering family work
- Offering individual therapy to family members
What happens after such early intervention?
Early intervention results in many people making a full recovery within two years and do not need follow-up from another mental health service, with their care being returned to their GP.
For others, the recovery process takes longer than two years, and their care is transferred to a local community-based Mental Health Team for further support.
“My memories from the first month of this episode are fairly hazy”
Early Intervention in First Episode Psychosis: A Service User’s Experience
Stephanie Allan; Early Intervention in First Episode Psychosis: A Service User’s Experience, Schizophrenia Bulletin, Volume 43, Issue 2, 1 March 2017, Pages 234–235, https://doi.org/10.1093/schbul/sbv227
Video on Psychosis and how early intervention can help… courtesy of EPUT – Essex Partnership University NHS Foundation Trust
Further information and support
Be informed! These sites can help you learn more about…
What is psychosis?
Maudsley NHS video What is psychosis?
Help for psychosis
The British Psychological Society has written a report called ‘Understanding Psychosis and Schizophrenia’. It has lots of information about what it means to have psychosis and what can help. It has personal stories written by people who have experienced psychosis about what this has been like for them and what has helped.
You can read it here.
Medicines and their side effects
There are published guidelines about the standard of care it is reasonable to expect:
Local and national organisations
- Scottish Recovery Network
- Support in Mind Scotland
- Glasgow Association for Mental Health
- Breathing Space is an NHS helpline that offers emotional support for people experiencing low mood, depression or anxiety. They can be contacted on 0800 83 85 87. They are open Monday to Thursday between 6pm and 2am and Saturday and Sunday between 6pm and 6am.
- See Me Scotland can help you find out more about the stigma of mental illness, and what you can do to stop it in Scotland.
- The Mental Health Act in Scotland, Advance Statements, and your legal rights.
BSL – Psychosis
NHSGG&C BSL A-Z: Mental Health – Psychosis
Psychosis is a term used to describe a number of unusual experiences:
- hearing or seeing things that other people can’t hear or see (hallucinations)
- holding unusual beliefs that people from a similar background would think strange or irrational (this includes delusions and paranoia)
- being so jumbled in thoughts or speech that other people can’t easily make sense of what you are meaning (thought disorder)
- experiencing periods of confusion – for example: becoming very distracted and finding it difficult to pay attention or make decisions
Psychosis can happen to anyone, up to 10 per cent of people will at some point in their life hear a voice talking to them when there is no-one there. Lots of things can contribute to a person experiencing psychosis such as stress, physical illnesses, using drugs or alcohol and mental illnesses
NHSGG&C BSL A-Z: Mental Health – Schizophrenia
Schizophrenia is a serious mental illness that affects thinking, emotions and behaviour. It is the most common form of psychosis. Schizophrenia usually affects people for the first time when they reach early adulthood – from their late teens to early thirties. Symptoms include:
- Hallucinations – hearing, smelling, feeling or seeing something that isn’t there.
- Delusions – believing something completely even though others find your ideas strange and can’t work out how you’ve come to believe them.
- Difficulty thinking – you find it hard to concentrate and tend to drift from one idea to another. Other people can find it hard to understand you.
- Feeling controlled – you may feel that your thoughts are vanishing, or that they are not your own, or that your body is being taken over and controlled by someone else.
Other symptoms include:
- Loss of interest, energy and emotions.
- Problems with motivation and organising yourself.
Problems with routine jobs like washing, tidying, or looking after yourself
Please note that this video is from a range of BSL videos published by NHS Greater Glasgow & Clyde
BSL – Anti-Psychotic Medication
NHSGG&C BSL A-Z: Mental Health – Anti-Psychotic Medication
Anti-Psychotic Medications are an important part of treatment for psychosis. They may need to be taken for a long time to keep well. There are different types of anti-psychotic medication and they can be taken as tablets, injections or as a liquid
Please note that this video is from a range of BSL videos published by NHS Greater Glasgow & Clyde