The Equality & Human Rights Team offers a range of training opportunities for staff members.
In addition to our scheduled training courses, we make every effort to respond to specific requests from staff groups. In order to ensure that we have sufficient information to do this, please consider the following before completing the request form.
Purpose of Training
It is important to be clear about what you wish to achieve with your training request, such as policy compliance, service improvement or staff development. Please ensure training is:
• Approved via relevant NHSGGC management structures
• Documented in line with governance standards
• Linked to Staff PDPs and eKSF updates
Please note that training should not replace relevant HR practice and procedure. If there are concerns about conduct or live investigations outstanding, this is a matter for the Human Resources Department. For further information, go to the HR Connect Equality, Diversity and Inclusion webpage.
Training Content
You will be asked to specify the topics, competencies or behaviours to be covered in your training. For example: EQIA Lead Reviewer Training; Human Library; Equality Act overview; Communication Support; BSL Act; Anti-racism Plan.
For further information about our current equalities work, legislation and resources, please go to NHSGGC – Equalities in Health
Location & Registration
It is the requester’s responsibility to provide a suitable venue for training to be delivered. Please ensure availability of equipment and facilities for the agreed training delivery, such as a projector for PowerPoint or breakout space as required. Please note it is also the requester’s responsibility to manage course registration.
Evaluation
Course evaluation should be in place,such aspre/post assessments, feedback forms, observation or peer review.
Submit request
To submit a training request, please complete the online form. A member of the Equality & Human Rights Team will be in touch to discuss your request.
Was this helpful?
Yes
No
Thanks for your feedback!
We want to ensure that all our patients have access to the right care in the right place at the right time. This means making sure that everyone understands the range of services available in order to decide what best meets their needs.
Many patients with protected characteristics can experience barriers to receiving the care they need. These include a lack of accessible information explaining the emergency care system, difficulties understanding and working their way through the appointments system and problems managing online or telephone support.
A&E departments are often the only service people are aware of that they can walk into to get help when they are worried and in pain. This means that they are often in the wrong place to get the proper care for their ailment. It is therefore vital to provide accessible information and routes to care for those who don’t know the system.
Working with protected characteristic groups
We are liaising with our emergency departments and charities to create opportunities to engage directly with protected characteristic groups. We will work with them to –
Create accessible resources that describe routes into our services and the alternatives to emergency care
Capture people’s experiences of accessing the right care in the right place to use as case studies
Help us support our emergency services to meet the needs of people with protected characteristics
Was this helpful?
Yes
No
Thanks for your feedback!
Digital solutions are making access to health care easier for many people. However, for some people, they are creating additional barrier to accessing care.
Also, where traditional routes into services are being replaced by digital ones, there may be a negative impact on people with certain protected characteristics – such as age, disability and race.
For example Glasgow Disability Alliance’s ‘Disabled People’s Mental Health Matters’ report (2021) highlighted that of the 2,500 disabled people involved, 1,500 faced digital exclusion with no access to devices, Wi-Fi or lacking the confidence to use it.
We want to ensure that these changes to the way patients access care will not disadvantage anyone who is digitally excluded. To this end, we are assessing the impact of all proposed service redesigns where digital solutions feature as alternatives to pre-existing care pathways. We are also engaging with protected characteristic groups to better understand their experience of using digital routes into services and will make appropriate adjustments.
Was this helpful?
Yes
No
Thanks for your feedback!
NHSGGC is committed to improving the experiences and health outcomes for patients with a learning disability (LD).
Our Acute Learning Disability and Autism Group leads this programme of activity and is working with local LD groups, patients, carers and families to improve hospital inpatient experiences.
This work includes a focus on –
Improved admission process, including providing thorough background information/ hospital passport
Reduced length of stay
Reduced hospital complications
Greater Carer involvement.
Autistic and Neurodivergent people experience some of the greatest inequalities in society
It is estimated that one in 100 people in Scotland are Autistic or Neurodivergent. There are many reasons why Autistic people may face barriers in accessing healthcare, including the following –
Executive functioning differences such as working memory, decision making and time management can lead to professionals to perceive Autistic people as being unwilling to engage with services or not requiring them.
Autistic people are very likely to experience the sensory world in a different way and healthcare environments have unusual smells, noises and lighting. These sensory differences may also be increased if the person is anxious or stressed.
A lack of understanding and stigma felt by Autistic people when engaging with services can lead to attempts to mask autistic symptoms which can lead to poor patient experience.
Everyone’s experience of being autistic is different, so it’s vital that all our staff understand the importance of a person-centred approach. There are lots of different kinds of reasonable adjustments that can be put in place which could greatly improve patient experience.
Activities include –
The introduction of an Autism Passport that can be shared between patients and staff. This will explain what should be considered when delivering care
Supporting Autistic and Neurodivergent people to sense check services as part of our Disability Discrimination Audits
The production of an Autism and Neurodivergence patient pathway app to provide easy access, useful information for staff.
Was this helpful?
Yes
No
Thanks for your feedback!
Shqip (Albanian)
Sigurohuni që po merrni kujdesin e duhur në vendin e duhur
Shkoni në Departamentin e Urgjences vetëm nëse keni nevojë për kujdes urgjent për një urgjencë të tillë si një sulm i dyshuar në zemër, goditje në tru ose gjakderdhje të tepërt. Nëse kjo është rasti, thirrni 999 duke përdorur shërbimin tonë të përkthimit me telefon.
Nëse shkoni në Departamentin e Urgjences me simptoma të tjera, mund të refuzoheni dhe të dërgoheni diku tjetër nëse nuk jeni në vendin e duhur për të marrë kujdesin e duhur. Nëse qëndroni, do të prisni një kohë shumë të gjatë pasi kushdo me një gjendje më urgjente do të shihet gjithmonë i pari, edhe nëse ka ardhur pas jush.
Nëse mendoni se duhet të shkoni në A&E, por nuk është kërcënuese për jetën, telefononi NHS24 falas në 111
Ju mund ta bëni këtë duke përdorur shërbimin tonë të përkthimit telefonik. NHS24 do t’ju ndihmojë të merrni kujdesin e duhur mjekësor në vendin e duhur, shpesh më afër shtëpisë dhe pa pasur nevojë të shkoni në Departamentin e Urgjences. Për shembull, mund të referoheni në një klinikë lëndimesh të vogla ose të bëni një video-telefonatë me një mjek.
تأكد من حصولك على الرعاية المناسبة في المكان المناسب
لا تذهب إلى قسم الطوارئ إلا إذا كنت بحاجة إلى رعاية عاجلة لحالة طارئة مثل نوبة قلبية مشتبه بها أو سكتة دماغية أو نزيف مفرط. إذا كان الأمر كذلك، فاتصل بالرقم 999 باستخدام خدمة الترجمة عبر الهاتف.
إذا ذهبت إلى قسم الطوارئ مع أعراض أخرى، فقد يتم رفضك وإرسالك إلى مكان آخر إذا لم تكن في المكان المناسب للحصول على الرعاية الصحيحة. إذا بقيت، فستنتظر لفترة طويلة جدًا حيث سيتم دائمًا رؤية أي شخص يعاني من حالة أكثر إلحاحًا أولاً، حتى لو جاء بعدك.
إذا كنت تعتقد أنك بحاجة إلى الذهاب إلى قسم الطوارئ و لكنها ليست مهددة للحياة، فاتصل بـ NHS24 مجانًا على 111
يمكنك القيام بذلك باستخدام خدمة الترجمة عبر الهاتف. ستساعدك NHS24 في الحصول على الرعاية الطبية المناسبة في المكان المناسب، وغالبًا ما تكون أقرب إلى المنزل ودون الحاجة إلى الذهاب إلى قسم الطوارئ. على سبيل المثال، يمكن إحالتك إلى عيادة إصابات طفيفة أو إجراء مكالمة فيديو مع الطبيب.
নিশ্চিত করুন যে আপনি সঠিক জায়গায় সঠিক যত্ন পাচ্ছেন।
সন্দেহজনক হার্ট অ্যাটাক, স্ট্রোক বা অতিরিক্ত রক্তপাতের মতো জরুরি অবস্থার জন্য যদি আপনার জরুরি চিকিৎসার প্রয়োজন হয়, তবেই কেবল জরুরি বিভাগে যান। যদি এমন হয়, তাহলে আমাদের টেলিফোন দোভাষী পরিষেবা ব্যবহার করে 999 নম্বরে কল করুন।
যদি আপনি অন্যান্য লক্ষণ নিয়ে জরুরি বিভাগে যান, তাহলে সঠিক যত্ন নেওয়ার জন্য সঠিক জায়গায় না থাকলে আপনাকে ফিরিয়ে দেওয়া হতে পারে এবং অন্য কোথাও পাঠানো হতে পারে। যদি আপনি থেকে যান, তাহলে আপনাকে অনেকক্ষণ অপেক্ষা করতে হবে কারণ জরুরি অবস্থার সাথে জড়িত যে কাউকেই সবসময় প্রথমে দেখা হবে, এমনকি যদি তারা আপনার পরে আসে।
যদি আপনার মনে হয় আপনার জরুরি বিভাগে যাওয়া উচিত কিন্তু এটি জীবনের জন্য হুমকিস্বরূপ নয়, তাহলে NHS24-কে 111 নম্বরে বিনামূল্যে কল করুন।
আপনি আমাদের টেলিফোন দোভাষী পরিষেবা ব্যবহার করে এটি করতে পারেন। NHS24 আপনাকে সঠিক জায়গায় সঠিক চিকিৎসা সেবা পেতে সাহায্য করবে, প্রায়শই বাড়ির কাছাকাছি এবং জরুরি বিভাগে যাওয়ার প্রয়োজন ছাড়াই। উদাহরণস্বরূপ, আপনাকে একটি ছোটখাটো আঘাতের ক্লিনিকে রেফার করা যেতে পারে অথবা একজন ডাক্তারের সাথে ভিডিও কল করতে পারেন।
Уверете се, че Получавате Правилната Помощ на Правилното Място
Отидете в спешното отделение, само ако се нуждаете от спешна помощ, като например инфаркт, инсулт или обилно кървене. Ако случаят е такъв, обадете се на 999 като използвате нашата услуга за превод по телефона.
Ако отидете в спешното отделение с други симптоми, може Ви изпратят някъде другаде, ако не сте на най-подходящото място, за да Ви се окаже правилната медицинска помощ. Ако останете в спешното отделение, е възможно да чакате дълго време, защото ако хора с по-животозастрашаващо състояние дойдат, те ще бъдат прегледани първи, дори и да са дошли след вас.
Ако смятате, че трябва да отидете в спешното отделение, но състоянието Ви не е животозастрашаващо, се обадете безплатно 24 часа в денонощието на линията за помощ към Националната Здравна Служба на телефон 111
Можете да се възползвате от услугата за преводач по телефона. 24-часовата линия за помощ към Националната Здравна Служба ще ви помогне да получите правилната медицинска помощ на правилното място, много често по-близо до дома Ви без да трябва да отивате в спешното отделение. Например, може да бъдете насочени към спешна клиника или да Ви бъде организирана видео консултация с лекар.
Ujistěte se, že dostáváte správnou péči na správném místě.
Na pohotovost choďte pouze v případě naléhavé péče, například při podezření na infarkt, mrtvici nebo nadměrné krvácení. V takovém případě zavolejte na číslo 999 s využitím naší telefonní tlumočnické služby.
Pokud půjdete na pohotovost s jinými příznaky, mohou vás odmítnout a poslat jinam, pokud nejste na správném místě, kde můžete dostat správnou péči. Pokud zůstanete, budete čekat velmi dlouho, protože každý, kdo má naléhavější stav, bude vždy ošetřen dříve, i když přišel po vás.
Pokud si myslíte, že musíte jít na pohotovost, ale není to život ohrožující, zavolejte zdarma na NHS24 na číslo 111.
Můžete to udělat pomocí naší telefonní tlumočnické služby. NHS24 vám pomůže získat správnou lékařskou péči na správném místě, často blíže k vašemu domovu, a bez nutnosti jít na pohotovost. Například vás mohou poslat na kliniku pro menší zranění nebo si můžete domluvit videohovor s lékařem.
Make Sure You Are Getting the Right Care in the Right Place
Only go to the Emergency Department if you need urgent care for an emergency such as a suspected heart attack, stroke or excessive bleeding. If this is the case, call 999 using our telephone interpreting service.
If you go to the Emergency Department with other symptoms, you may be turned away and sent elsewhere if you are not in the right place to get the correct care. If you do stay, you will be waiting a very long time as anyone with a more urgent condition will always be seen first, even if they came in after you.
If you think you need to go to the Emergency Department but it is not life threatening call NHS24 free on 111
You can do this using our telephone interpreting service. NHS24 will help you get the right medical care in the right place, often closer to home and without the need to go to the Emergency Department. For example you could be referred to a minor injury clinic or have a video call with a doctor.
مطمئن شوید که شما مراقبت مناسب را در مکان مناسب دریافت میکنید
فقط در صورتی به بخش عاجل مراجعه کنید که برای یک حالت اضطراری مانند حمله قلبی مشکوک، سکته یا خونریزی بیش از حد نیاز به مراقبت فوری دارید. اگر این قضیه باشد، با استفاده از خدمات ترجمه تلیفون ما با 999 تماس بگیرید.
اگر شما با علایم دیگر به بخش عاجل بروید، اگر شما در جای مناسب برای دریافت مراقبت درست نباشید، ممکن است شما را رد کرده و به جای دیگری فرستاده شوید. اگر شما بمانید، شما برای مدت طولانی منتظر خواهید بود زیرا هر کسی که یک حالت عاجل تر داشته باشد همیشه اول دیده خواهد شد، حتی اگر آنها بعد از شما بیایند.
اگر شما فکر میکنید که شما باید به بخش عاجل بروید مگر این تهدید کننده زندگی نیست با NHS24 رایگان به شماره 111 تماس بگیرید
شما میتوانید این کار را با استفاده از خدمات ترجمانی تلیفون ما انجام دهید. NHS24 به شما کمک خواهد کرد تا مراقبت طبی مناسب را در مکان مناسب، اغلب اوقات نزدیک به خانه و بدون نیاز به رفتن به بخش عاجل بدست بیاورید. بطور مثال شما ممکن به یک کلینیک آسیب های جزئی معرفی شوید یا با یک داکتر یک تماس ویدیویی داشته باشید.
برای ساخت (Farsi)
اطمینان حاصل کنید که مراقبت مناسب را در محل مناسب دریافت میکنید
تنها در صورتی به بخش اورژانس مراجعه کنید که نیاز به مراقبت فوری برای یک وضعیت اضطراری مانند احتمال حمله قلبی، سکته مغزی یا خونریزی شدید، دارید. در چنین شرایطی، با استفاده از خدمات مترجمی تلفنی ما با شماره999 تماس بگیرید.
اگر با علائم دیگری به بخش اورژانس مراجعه کنید، ممکن است پذیرش نشوید و به مرکزی هدایت شوید که مراقبت مناسبتری ارائه میدهد. حتی اگر بمانید، باید مدت بسیار طولانی منتظر بمانید، زیرا همیشه افرادی که وضعیت اضطراریتری دارند، حتی اگر بعد از شما مراجعه کرده باشنددر اولویت قرار میگیرند.
اگر فکر میکنید باید به بخش اورژانس مراجعه کنید اما وضعیت شما تهدیدکننده زندگی نیست، با شماره 111 و بهصورت رایگان با خدمات درمانی ۲۴ ساعته (NHS 24) تماس بگیرید.
میتوانید این کار را با استفاده از خدمات مترجمی تلفنی ما انجام دهید. خدمات درمانی ۲۴ ساعته (NHS 24) به شما کمک میکند مراقبت پزشکی مناسب را در مکان درست و اغلب در نزدیکی خانهتان دریافت کنید، بدون اینکه لازم باشد به بخش اورژانس مراجعه کنید. برای مثال، ممکن است به یک کلینیک آسیبهای جزئی ارجاع داده شوید یا یک مشاوره ویدیویی با پزشک داشته باشید.
Assurez-vous de recevoir le traitement approprié au bon endroit.
Ne vous rendez au service des urgences que si vous avez besoin d’une prise en charge immédiate pour une urgence, comme une suspicion de crise cardiaque, d’accident vasculaire cérébral ou d’hémorragie grave. Si tel est le cas, veuillez appeler le 999 et demander notre service d’interprétation téléphonique.
Si vous vous rendez au département des urgences avec des symptômes qui ne correspondent pas à votre situation, vous pouvez être refusé et orienté vers un autre établissement. Si vous choisissez de rester, soyez prêt à attendre longtemps. Les cas urgents sont toujours prioritaires, même si la personne arrive après vous.
Si votre situation n’est pas vitale, appelez gratuitement le NHS24 au 111 avant de vous rendre au département des urgences.
Pour bénéficier de soins médicaux adaptés, utilisez notre service d’interprétation téléphonique. NHS24 vous guide vers le lieu de traitement le plus approprié, souvent près de chez vous, vous évitant ainsi de vous rendre aux urgences. Par exemple, on peut vous orienter vers une clinique pour des blessures légères ou organiser une consultation vidéo avec un médecin.
დარწმუნდით, რომ შესაბამის მკურნალობას იტარებთ შესაბამის ადგილზე.
მიმართეთ სასწრაფო გადაუდებელი დახმარების განყოფილებას მხოლოდ მაშინ, როცა გადაუდებელი მკურნალობა გესაჭიროებათ, ისეთი სასწრაფო მდგომარეობისას, როგორიცაა გულის შეტევა, ინსულტი ან ძლიერი სისხლდენა. თუ ეს სიტუაციაა, მაშინ დარეკეთ 999-ზე და ისარგებლეთ სატელეფონო თარჯიმნის მომსახურებით.
თუ თქვენ მიმართავთ სასწრაფო გადაუდებელი დახმარების განყოფილებას სხვა სიმპტომებით, შეიძლება არ მიგიღონ და გადაგამისამართონ სხვა ადგილზე, იმის გამო. რომ ეს ადგილი არ შეესაბამებოდეს თქვენს მდგომარეობას. თუ აქ დარჩებით, თქვენ მოგიწევთ დიდი ხნით ლოდინი, რადგან ჯერ იმ პაციენტებს მოემსახურებიან, რომლებსაც უფრო სერიოზული მდგომარეობა აქვთ, თუნდაც თქვენს შემდეგ იყვნენ რიგში.
თუ ფიქრობთ, რომ გჭირდებათ სასწრაფო გადაუდებელი დახმარების განყოფილებაში წასვლა, მაგრამ თქვენი მდგომარეობა სიცოცხლისთვის საშიში არ არის, უფასოდ დარეკეთ NHS24-ზე (შოტლანდიის ეროვნული სატელეფონო ჯანდაცვისა და სატელეფონო მეთვალყურეობის ორგანიზაცია) ნომერზე 111.
შეგიძლიათ ისარგებლოთ სატელეფონო თარჯიმნის სერვისით. NHS24 (შოტლანდიის ეროვნული სატელეფონო ჯანდაცვისა და სატელეფონო მეთვალყურეობის ორგანიზაცია) დაგეხმარებათ მიიღოთ შესაბამისი სამედიცინო დახმარება შესაბამის ადგილზე, ხშირად თქვენს სახლთან ახლოს და სასწრაფო გადაუდებელი დახმარების განყოფილებაში წასვლის გარეშე. მაგალითად, თქვენ შესაძლოა, გადაგამისამართონ მცირე ტრავმების კლინიკაში ან გქონდეთ ვიდეო ზარი ექიმთან.
Βεβαιωθείτε ότι λαμβάνετε τη σωστή φροντίδα στο σωστό μέρος
Πηγαίνετε στο Τμήμα Επειγόντων Περιστατικών μόνο εάν χρειάζεστε επείγουσα φροντίδα για έκτακτη ανάγκη, όπως υποψία καρδιακής προσβολής, εγκεφαλικού επεισοδίου ή υπερβολικής αιμορραγίας. Σε αυτή την περίπτωση, καλέστε το 999 χρησιμοποιώντας την τηλεφωνική υπηρεσία διερμηνείας μας.
Αν πάτε στο Τμήμα Επειγόντων Περιστατικών με άλλα συμπτώματα, μπορεί να σας απορρίψουν και να σας στείλουν αλλού, αν δεν βρίσκεστε στο σωστό μέρος για να λάβετε τη σωστή φροντίδα. Αν μείνετε, θα περιμένετε για πολύ καιρό, καθώς όποιος έχει πιο επείγουσα πάθηση θα εξετάζεται πάντα πρώτος, ακόμα κι αν ήρθε μετά από εσάς.
Αν νομίζετε ότι χρειάζεται να πάτε στο Τμήμα Επειγόντων Περιστατικών αλλά δεν υπάρχει κίνδυνος για τη ζωή σας, καλέστε δωρεάν το NHS24 στο 111
Μπορείτε να το κάνετε αυτό χρησιμοποιώντας την υπηρεσία τηλεφωνικής διερμηνείας μας. Το NHS24 θα σας βοηθήσει να λάβετε τη σωστή ιατρική περίθαλψη στο σωστό μέρος, συχνά πιο κοντά στο σπίτι και χωρίς να χρειάζεται να πάτε στο Τμήμα Επειγόντων Περιστατικών. Για παράδειγμα, θα μπορούσατε να παραπεμφθείτε σε μια κλινική ελαφρών τραυματισμών ή να έχετε μια βιντεοκλήση με έναν γιατρό.
सुनिश्चित करें कि आपको सही जगह पर सही देखभाल मिल रही है
केवल तभी आपातकालीन विभाग में जाएं जब आपको किसी आपातकालीन स्थिति के लिए तत्काल देखभाल की आवश्यकता हो, जैसे कि संदिग्ध हृदयाघात, स्ट्रोक या अत्यधिक रक्तस्राव। यदि ऐसा है, तो हमारी टेलीफोन अनुवादन सेवा का उपयोग करके 999 पर कॉल करें।
यदि आप अन्य लक्षणों के साथ आपातकालीन विभाग में जाते हैं, तो आपको वापस भेजा जा सकता है और किसी अन्य स्थान पर भेजा जा सकता है यदि आप उचित देखभाल प्राप्त करने के लिए सही स्थान पर नहीं हैं। यदि आप रुकते हैं, तो आपको बहुत लंबा इंतजार करना पड़ेगा, क्योंकि अधिक गंभीर स्थिति वाले व्यक्ति को हमेशा पहले देखा जाएगा, भले ही वे आपके बाद आए हों।
यदि आपको लगता है कि आपको आपातकालीन विभाग में जाने की आवश्यकता है, लेकिन यह जीवन के लिए खतरा नहीं है, तो NHS24 को 111 पर निःशुल्क कॉल करें
आप हमारी टेलीफोन व्याख्या सेवा का उपयोग करके ऐसा कर सकते हैं। NHS24 आपको सही जगह पर सही चिकित्सा सेवा पाने में मदद करेगा, अक्सर घर के करीब और बिना आपातकालीन विभाग में जाने की आवश्यकता के। उदाहरण के लिए आपको मामूली चोट वाले क्लिनिक में भेजा जा सकता है या डॉक्टर से वीडियो कॉल पर बात की जा सकती है।
Bizonyosodjon meg róla, hogy a megfelelő helyen kapja a megfelelő ellátást!
Csak akkor menjen a sürgősségi osztályra, ha sürgős ellátásra van szüksége vészhelyzet esetén, mint például feltételezett szívroham, stroke vagy erős vérzés. Ilyenkor hívja a 999-et telefonos tolmácsszolgálatunk segítségével!
Ha más tünetekkel megy a sürgősségi osztályra, előfordulhat, hogy – amennyiben nem a megfelelő helyen van – elküldik máshová, ahol megfelelő ellátást kaphat. Ha mégis marad, akkor nagyon sokáig kell várakoznia, mivel a sürgősebb állapotban lévőket mindig előbb látják el, még akkor is, ha azok Ön után érkeztek.
Ha úgy gondolja, hogy a sürgősségi osztályra kell mennie, de az állapota nem életveszélyes, hívja az NHS24-et ingyenesen a 111-es számon.
Ezt teheti a telefonos tolmácsszolgálatunk segítségével. Az NHS24 segít abban, hogy megfelelő egészségügyi ellátást kapjon a megfelelő helyen, gyakran közelebb az otthonához, anélkül, hogy sürgősségi osztályra kellene mennie. Például tovább irányíthatják egy kisebb sérüléseket ellátó klinikára, vagy videóhíváson keresztül konzultálhat orvossal.
Assicurati di ricevere le cure giuste nel posto giusto
Vai al pronto soccorso solo se hai bisogno di cure urgenti per un’emergenza come un sospetto infarto, ictus o sanguinamento eccessivo. In tal caso, chiamate il 999 utilizzando il nostro servizio di interpretariato telefonico.
Se vai al pronto soccorso con altri sintomi, potresti essere allontanato e mandato altrove se non sei nel posto giusto per ottenere le cure corrette. Se rimani, aspetterai molto tempo poiché chiunque abbia una condizione più urgente verrà sempre visto per primo, anche se è venuto dopo di te.
Se pensi di dover andare al pronto soccorso ma non sei in pericolo di vita, chiama NHS24 gratuitamente al 111
Puoi farlo utilizzando il nostro servizio di interpretariato telefonico. NHS24 ti aiuterà a ottenere le giuste cure mediche nel posto giusto, spesso più vicino a casa e senza la necessità di andare al pronto soccorso. Ad esempio, potresti essere indirizzato a una clinica per lesioni minori o fare una videochiamata con un medico.
Mek shor say yu dae get di rait kɛa na di rait plas
Onli go Imɛrjɛnsi Dipatmɛnt if yu nid urjɛnt kɛa fɔ wan ɛmɛrjɛnsi lɛk wan suspekt way gɛt hɑt attak,
strok ɔ excessive blɛdɪn. If dis na di kas, kol 999 yus wi telefon intɛprɛt sɑvis.
If yu go Imɛrjɛnsi Dipatmɛnt wit ɔda simptɔm, dɛm kin sɛn yu away ɔda sai if yu nɔ dae na di rait plas fɔ gɛt di kɔrɛkt kea. If yu stay, yu go dae wait fɔ vɛri long tɛm as enibɔdi wae gɛt mōre urjɛnt kondishon go dae si fɔs, ɛn ɛven if dɛm kam in afta yu.
If yu tink yu nɛd fɔ gɔ to Imɛrjɛnsi Dipatmɛnt but norto lyfe thrɛtɛn kɔl NHS24 frɛ na 111
Yɔ kin du dis yuzin a telɛfɔn intɛrpritin savis. NHS24 go hɛp yu fɔ gɛt di rait mɛdikal kɛa na di rait plas, ɔftɛn klɔs na hɔm ɛn witɔut di nid fɔ gɔ na Imɛrjɛnsi Dipatmɛnt. Fɔ ɛksɛmpl, yu fit bɛ rɛfɛrd to d maɪnɔ injuri klɪnɪk ɔr gɛt a video kɔl wit a dɔkta.
Pārliecinieties, ka saņemat pareizo aprūpi pareizajā vietā.
Dodieties uz Neatliekamās palīdzības nodaļu tikai tad, ja jums nepieciešama steidzama palīdzība, piemēram, ja ir aizdomas par sirdslēkmi, insultu vai pārmērīgu asiņošanu. Šajā gadījumā zvaniet 999, izmantojot mutiskās tulkošanas pakalpojumu.
Ja vērsīsieties Neatliekamās palīdzības nodaļā ar citiem simptomiem, jums iespējams tiks atteikta palīdzība un jūs nosūtīs citur, jo neatradīsieties pareizajā vietā, kur jums var tikt sniegta atbilstoša aprūpe. Ja jūs tomēr paliksiet, jūs gaidīsiet ļoti ilgi, jo visi, kam ir steidzamāka slimība, vienmēr tiks pieņemti pirmie, pat ja viņi ieradīsies pēc jums.
Ja domājat, ka jums jādodas uz uz Neatliekamās palīdzības nodaļu , bet jūsu dzīvība nav apdraudēta, zvaniet NHS24 pa bezmaksas tālruni 111.
To varat izdarīt pa tālruni, izmantojot mūsu mutiskās tulkošanas pakalpojumu. NHS24 palīdzēs jums saņemt pareizo medicīnisko aprūpi pareizajā vietā, bieži vien tuvāk mājām un bez nepieciešamības doties uz Neatliekamās palīdzības nodaļu. Piemēram, jūs varētu nosūtīt uz nelielu traumu klīniku vai veikt videozvanu ar ārstu.
Sala nyonso mpo Ozwa Soins ya malamu na esika ebongi
Kende kaka na Emergency Department soki ozali na mposa ya lisalisi ya nokinoki mpo na likambo ya mbalakaka lokola oyo bakanisaka ete bazali na bokono ya motema, AVC, to kobima makila ebele. Soki ezali bango benga 999 kosalela service na biso y aba interpreters na telepone.
Soki okeyi na Emergency Department na bokono mosusu, bakoki kozongisa yo to mpe kotinda yo esika mosusu soki ozalaki na esika ya malamu te mpo na kozwa lisalisi. Soki otie moto makasi otikali, okozela ntango molayi mpamba, pe moto nyonso oyo azali na bokono ya monene bako yamba ye na lombango mpe liboso, ata soki ayaki na nsima na yo.
Soki okanisi ete osengeli kokende na Emergency Department kasi ezali na likama ya bomoyi mpe kufa te, benga NHS24 ofele na 111
Okoki kosala yango na lisungi ya ba interpretre na biso na telefone. Benga NHS24 bakosalisa yo ozwa lisungi ya monganga ya malamu na esika ya esengeli, mbala mingi ekoki kosala penepene na ndako na bongo tina ya kokenge na Emergency Department ekosala te. Na ndakisa, bakoki kotinda yo na kliniki to kobengela yo monganga na nzela ya video.
Įsitikinkite, kad gaunate tinkamą priežiūrą tinkamoje vietoje
Važiuokite į Skubiąją pagalbą tik tuo atveju, jei jums reikia skubios pagalbos dėl neatidėliotinos pagalbos, pvz., įtariamo širdies priepuolio, insulto ar gausaus kraujavimo.
Jei kreipiatės į Skubiąją pagalbą su kitais simptomais, galite būti nepriimti ir išsiųsti kitur, kur būtų tinkama vieta, kad gautumėte priežiūrą. Jei pasiliksite, lauksite labai ilgai, nes visi, kurių būklė sunkesnė, visada bus matomi pirmieji, net jei jie ateis vėliau po jūsų.
Jei manote, kad jums reikia kreiptis į Skubiąją pagalbą, bet tai nekelia pavojaus gyvybei, skambinkite NHS24 nemokamu numeriu 111
Tai galite padaryti naudodami mūsų vertimo žodžiu paslaugą telefonu. NHS24 padės gauti reikiamą medicininę priežiūrą reikiamoje vietoje, dažnai arčiau namų ir nereikia vykti į Skubią pagalbą. Pavyzdžiui, galite būti nukreipti į nedidelių sužalojimų kliniką arba gauti vaizdo pokalbį su gydytoju.
Upewnij się, że otrzymujesz właściwą opiekę we właściwym miejscu
Udaj się na szpitalny oddział ratunkowy tylko wtedy, gdy potrzebujesz pilnej opieki w nagłych przypadkach, takich jak podejrzenie zawału serca, udar mózgu lub nadmierne krwawienie. W takich sytuacjach zadzwoń pod numer 999, korzystając z naszej usługi tłumaczenia telefonicznego.
Jeśli zgłosisz się na szpitalny oddział ratunkowy z innymi objawami, możesz zostać odesłany/-a w inne miejsce, w którym będziesz mógł/mogła skorzystać z odpowiedniej opieki. Jeśli zostaniesz na oddziale, spędzisz bardzo długi czas w oczekiwaniu na wizytę, ponieważ osoby z bardziej pilnymi dolegliwościami zawsze będą przyjmowane w pierwszej kolejności, nawet jeśli zgłosiły się do szpitala po Tobie.
Jeśli uważasz, że musisz udać się na szpitalny oddział ratunkowy, ale stan, w jakim się znajdujesz, nie zagraża Twojemu życiu, zadzwoń pod bezpłatny numer NHS24 111.
Możesz to zrobić, korzystając z naszej usługi tłumaczenia telefonicznego. NHS24 pomoże Ci skorzystać z właściwej opieki medycznej we właściwym miejscu, często bliżej domu i bez konieczności udawania się na szpitalny oddział ratunkowy. Możesz na przykład zostać skierowany/-a do poradni leczenia drobnych urazów lub umówić się na wideorozmowę z lekarzem.
Certifique-se de que está recebendo o tratamento adequado no local correto.
Dirija-se ao Serviço de Urgência somente se precisar de atendimento imediato por uma emergência, como suspeita de ataque cardíaco, AVC ou hemorragia grave. Se for esse o caso, ligue para o 112 e solicite o nosso serviço de interpretação telefônica.
Se você for ao Departamento de Emergência com sintomas que não sejam adequados à sua condição, poderá ser recusado e encaminhado para outro local. Caso decida permanecer, esteja preparado para uma longa espera, pois aqueles com necessidades mais urgentes sempre têm prioridade e serão atendidos primeiro, mesmo que tenham chegado depois de você.
Caso ache que necessita de se dirigir ao Departamento de Emergência, mas não se trata de uma situação de risco de vida, ligue gratuitamente para o NHS24 pelo número 111.
Para aceder a cuidados médicos adequados, poderá utilizar o nosso serviço de interpretação por telefone. O NHS24 ajuda a encaminhá-lo para o local de tratamento mais adequado e, muitas vezes, mais próximo da sua residência, evitando, assim, uma ida ao serviço de urgências. Por exemplo, poderá ser encaminhado para uma clínica de pequenos ferimentos ou realizar uma consulta por vídeo com um médico.
Asigura-te că primești îngrijirea potrivită la locul potrivit
Mergeți la Departamentul de Urgență dacă aveți nevoie de îngrijire urgentă pentru o urgență, cum ar fi o suspiciune de infarct miocardic, accident vascular cerebral sau sângerare excesivă. În acest caz, sunați la 999 folosind serviciul nostru de interpretare telefonică.
Dacă mergeți la Departamentul de Urgență cu alte simptome, este posibil să fiți întors și trimis în altă parte dacă nu vă aflați în locul potrivit pentru a primi îngrijirea corectă. Dacă rămâneți, veți aștepta foarte mult timp, deoarece oricine are o afecțiune mai urgentă va fi întotdeauna consultat primul, chiar dacă a venit după dumneavoastră.
Dacă credeți că trebuie să mergeți la Departamentul de Urgență, dar nu vă pune viața în pericol, sunați gratuit la NHS24 la 111.
Puteți face acest lucru folosind serviciul nostru de interpretare telefonică. NHS24 vă va ajuta să obțineți îngrijirea medicală potrivită la locul potrivit, adesea mai aproape de casă și fără a fi nevoie să mergeți la Departamentul de Urgență. De exemplu, ați putea fi trimis la o clinică pentru vătămări minore sau ați putea avea un apel video cu un medic.
Убедитесь, что вы получаете правильную медицинскую помощь в нужном месте
Обращайтесь в Отделение Неотложной Помощи (Emergency Department) только в случае экстренной необходимости, например, при подозрении на сердечный приступ, инсульт или сильное кровотечение. В этом случае звоните 999, используя наш телефонный сервис перевода.
Если вы придёте в Отделение Неотложной Помощи с другими симптомами, вас могут отправить в другое место, если это не подходящее место для получения правильной помощи. Если вы останетесь, вам придётся долго ждать, так как пациенты с более серьёзными и срочными состояниями будут обслужены первыми, даже если они пришли после вас.
Если вы считаете, что вам нужно обратиться в отделение неотложной помощи, но ситуация не угрожает жизни, звоните в NHS24 бесплатно по номеру 111.
Вы можете воспользоваться телефонным сервисом перевода. NHS24 поможет вам получить правильную медицинскую помощь в нужном месте, чаще всего ближе к дому и без необходимости идти в Отделение Неотложной Помощи. Например, вас могут направить в клинику для мелких травм или организовать видеозвонок с врачом.
Uistite sa, že dostávate správnu starostlivosť na správnom mieste.
Na pohotovosť choďte iba v prípade naliehavej starostlivosti, ako je podozrenie na infarkt, mŕtvicu alebo nadmerné krvácanie. V takom prípade zavolajte na číslo 999 s použitím našej telefonickej tlmočníckej služby.
Ak pôjdete na pohotovosť s inými príznakmi, môžu vás odmietnuť a poslať na iné miesto, ak nie ste na správnom mieste, kde môžete získať správnu starostlivosť. Ak zostanete, budete čakať veľmi dlho, pretože každý, kto má naliehavejší stav, bude vždy ošetrený skôr, aj keď prišiel po vás.
Ak si myslíte, že musíte ísť na pohotovosť, ale nie je to život ohrozujúce, zavolajte na bezplatnú linku NHS24 na čísle 111.
Môžete tak urobiť pomocou našej telefónnej tlmočníckej služby. NHS24 vám pomôže získať správnu lekársku starostlivosť na správnom mieste, často bližšie k vášmu domovu a bez potreby ísť na pohotovosť. Napríklad vás môžu poslať do kliniky pre menšie zranenia alebo si môžete dohodnúť videohovor s lekárom.
Hubi in aad ka Heleyso Daryeelka Saxda ah oo aad ka heleyso Goobta Saxda ah
Kaliya tag Qeybta Xaalada Degdegga ah haddii aad u baahan tahay daryeel degdeg ah xaalad degdeg ah sida wadne xanuunka la tuhunsan yahay, istaroog/faaliga ama dhiig-bax xad-dhaaf ah. Haddii aad sidaas daremeyso, wac 999 adigoo adeegsanaya adeegeyna turjumaadda telefoonka.
Haddii aad u tagto Qeybta Xaalada Degdegga ah oo leh astaamo kale, waxaa laga yaabaa in lagu celiyo oo meel kale laguu diro haddii aadan joogin meesha saxda ah si aad u hesho daryeelka saxda ah. Haddii aad joogtid, waxaad sugi doontaa wakhti aad u dheer maadaama qof kasta oo xaalad degdeg ah leh mar walba la arki doono marka hore, xitaa haddii ay ku soo galeen adiga dabadiis.
Haddii aad u malaynayso inaad u baahan tahay inaad aado Qeybta Xaalada Degdegga ah laakiin ayansan ahayn xalad nafta halis gelin karto wac NHS24 lambarka bilaashka ah 111
Waxaad taas ku samayn kartaa addoo isticmaalaya adeegayaga turjumaada telefoonka. NHS24 waxay kaa caawin doontaa inaad hesho daryeelka caafimaad ee saxda ah meesha saxda ah, inta badan guriga kuugu dhow oo aan u baahnayn inaad aado Qeybta Xaalada Degdegga ah. Tusaale ahaan waxaa laguu gudbin karaa rugta dhaawaca fudud ama waxaad la yeelan kartaa takhtar muuqaal ah.
Asegúrese de recibir la atención adecuada en el lugar adecuado
Acuda al servicio de urgencias sólo si necesita atención urgente por una emergencia como un presunto infarto de miocardio, un ictus o una hemorragia excesiva. Si es así, llama al 999 usando nuestro servicio de interpretación telefónica.
Si va al servicio de urgencias con otros síntomas, puede que le rechacen y le envíen a otro sitio si no está en el lugar adecuado para recibir la atención correcta. Si se queda, tendrá que esperar mucho tiempo, ya que siempre se atenderá primero a las personas con una enfermedad más urgente, aunque hayan llegado después que usted.
Si cree que necesita ir al servicio de urgencias pero su vida no corre peligro, llame gratis al NHS24 al 111
Puede hacerlo a través de nuestro servicio de interpretación telefónica. NHS24 le ayudará a recibir la atención médica adecuada en el lugar adecuado, a menudo más cerca de casa y sin necesidad de acudir al servicio de urgencias. Por ejemplo, puedes ser derivado a una clínica de lesiones leves o tener una videollamada con un médico.
Hakikisha unapata huduma inayofaa mahali panapofaa.
Unapaswa kwenda kwa Idara ya Ajali na Dharura pale tu unapohitaji huduma ya haraka kwa tatizo la dharura kama vile unaposhuku mshtuko wa moyo, kiharusi, au kutokwa na damu nyingi. Ikiwa hali ni hiyo, piga simu 999 ukitumia huduma yetu ya wakalimani wa simu.
Ukienda kwenye Idara ya Ajali na Dharura kwa matatizo mengine, unaweza kuambiwa uende sehemu nyingine ikiwa huko ndio mahali sahihi pa kupata huduma unayohitaji. Na hata ukikaa, utalazimika kusubiri kwa muda mrefu sana kwa sababu mgonjwa yeyote mwenye tatizo la dharura zaidi atapewa kipaumbele kwanza, hata kama amefika baada yako.
Ikiwa unafikiri unahitaji kwenda Idara ya Ajali na Dharura lakini hali yako si ya hatari kwa maisha, piga simu NHS24 bure kwa nambari 111.
Unaweza kutumia huduma yetu ya wakalimani wa simu kufanya hivyo. NHS24 itakusaidia kupata huduma sahihi ya matibabu mahali panapofaa, mara nyingi karibu na nyumbani kwako na bila kulazimika kwenda Idara ya Ajali na Dharura. Kwa mfano, unaweza kupelekwa kwenye kliniki ya majeraha madogo au kufanya mazungumzo ya video na daktari.
சரியான இடத்தில் சரியான பராமரிப்பைப் பெறுவதை உறுதிப்படுத்திக் கொள்ளுங்கள்.
சந்தேகிக்கப்படும் மாரடைப்பு, பக்கவாதம் அல்லது அதிக இரத்தப்போக்கு போன்ற அவசரநிலைக்கு அவசர சிகிச்சை தேவைப்பட்டால் மட்டுமே அவசர சிகிச்சைப் பிரிவுக்குச் செல்லவும். இதுபோன்ற நிலை ஏற்பட்டால், எங்கள் தொலைபேசி மொழிபெயர்ப்பு சேவையைப் பயன்படுத்தி 999 என்ற எண்ணை அழைக்கவும்.
நீங்கள் வேறு அறிகுறிகளுடன் அவசர சிகிச்சைப் பிரிவுக்குச் சென்றால், சரியான கவனிப்பைப் பெற நீங்கள் சரியான இடத்தில் இல்லையென்றால், நீங்கள் திருப்பி வேறு இடத்திற்கு அனுப்பப்படலாம். நீங்கள் காத்திருக்க முடிவு செய்தால், நீங்கள் மிக நீண்ட நேரம் காத்திருக்க வேண்டியிருக்கும், ஏனெனில் மிகவும் அவசரமான நிலையில் உள்ள எவரும் எப்போதும் முதலில் காணப்படுவார்கள், அவர்கள் உங்களுக்குப் பிறகு வந்தாலும் கூட.
நீங்கள் அவசர சிகிச்சைப் பிரிவுக்குச் செல்ல வேண்டும் என்று நினைத்தால், ஆனால் அது உயிருக்கு ஆபத்தானது அல்ல என்றால், 111 என்ற எண்ணில் NHS24 ஐ இலவசமாக அழைக்கலாம்.
எங்கள் தொலைபேசி மொழிபெயர்ப்பு சேவையைப் பயன்படுத்தி நீங்கள் இதைச் செய்யலாம். NHS24 உங்களுக்கு சரியான மருத்துவ சேவையை சரியான இடத்தில் பெற உதவும், பெரும்பாலும் இது வீட்டிற்கு அருகாமையில் இருக்கும், மேலும் அவசர சிகிச்சைப் பிரிவுக்குச் செல்ல வேண்டிய அவசியமும் இருக்காது. உதாரணமாக, நீங்கள் ஒரு சிறு கிளினிக்கு பரிந்துரைக்கப்படலாம் அல்லது ஒரு மருத்துவரிடம் வீடியோ அழைப்பு செய்யலாம்.
Sadece acil bir durum için, örneğin şüpheli kalp krizi, felç veya aşırı kanama gibi bir acil durumda Acil Servise (Emergency Department) gidin. Böyle bir durum söz konusuysa, telefon çeviri hizmetimizi kullanarak 999’u arayın.
Acil Servise başka semptomlarla giderseniz, doğru bakım alabileceğiniz yer uygun değilse sizi başka bir yere yönlendirebilirler. Eğer kalırsanız, çok uzun süre beklemeniz gerekir, çünkü daha acil durumu olan kişiler her zaman önce görülecektir, sizden sonra gelmiş olsalar bile.
Acil Servise gitmeniz gerektiğini düşünüyorsanız ancak durum hayati tehlike oluşturmuyorsa, NHS24’ü 111 numaradan ücretsiz arayın.
Bunu telefon çeviri hizmetimizi kullanarak yapabilirsiniz. NHS24, doğru tıbbi bakımı doğru yerde almanıza yardımcı olacaktır, genellikle eve daha yakın bir yerdeveAcil Servise gitmeye gerek kalmadan. Örneğin, sizi küçük yaralanmalar kliniğine yönlendirebilirveya bir doktorla görüntülü görüşme yapmanızı sağlayabilir.
Переконайтеся, що ви отримуєте правильну допомогу в правильному місці
Звертайтеся до відділення невідкладної допомоги лише у разі, якщо вам потрібна термінова допомога у зв’язку з таким надзвичайним станом, як підозра на інфаркт, інсульт або сильна кровотеча. У такому випадку зателефонуйте за номером 999, скориставшись нашою
послугою телефонного перекладу.
Якщо ви звернулися до відділення невідкладної допомоги з іншими симптомами, вас можуть відмовити і направити в інше місце, якщо ви не в тому місці, де вам нададуть належну медичну допомогу. Навіть якщо ви прийдете, вам доведеться чекати дуже довго, оскільки будь-кого з більш нагальними проблемами завжди приймають першими, навіть якщо вони прийшли після вас.
Якщо ви вважаєте, що вам потрібно звернутися до відділення невідкладної допомоги, але це не загрожує вашому життю, зателефонуйте безкоштовно до NHS24 за номером 111
Ви можете зробити це, скориставшись нашою послугою телефонного перекладу. NHS24 допоможе вам отримати потрібну медичну допомогу в потрібному місці, часто ближче до дому і без необхідності їхати до відділення невідкладної допомоги. Наприклад, вас можуть направити до клініки легких травм або організувати відеодзвінок з лікарем.
یقینی بنائیں کہ آپ کو صحیح جگہ پر صحیح دیکھ بھال مل رہی ہے۔
ایمرجنسی ڈیپارٹمنٹ صرف اس صورت میں جائیں جب آپ کو کسی ہنگامی صورت حال کے لیے فوری دیکھ بھال کی ضرورت ہو، مثال کے طور پر آپ کو دل کا دورہ پڑنے، فالج یا شدید خون بہنے کا شبہ ہو۔ اگر ایسا ہے تو، ہماری ٹیلی فون انٹرپریٹنگ سروس کا استعمال کرتے ہوئے 999 پر کال کریں۔
اگر آپ دیگر علامات کے ساتھ ایمرجنسی ڈیپارٹمنٹ جاتے ہیں، تو ہو سکتا ہے کہ آپ کو واپس بھیج دیا جائے او اگر آپ صحیح دیکھ بھال حاصل کرنے کے لیے صحیح جگہ پر نہیں ہیں تو کہیں اور بھیج دیا جائے۔ اگر آپ وہاں رکتے ہیں، تو آپ کو بہت طویل انتظار کرنا پڑے گا کیونکہ آپ سے زیادہ سنگین حالت سے دوچار شخص کو ہمیشہ پہلے دیکھا جائے گا، چاہے وہ آپ کے بعد ہی کیوں نہ آیا ہو۔
اگر آپ کو لگتا ہے کہ آپ کو ایمرجنسی ڈیپارٹمنٹ جانے کی ضرورت ہے لیکن یہ کوئی جان لیوا وجہ نہیں ہے، تو NHS24 کو 111 پر مفت کال کریں۔
آپ یہ کال ہماری ٹیلی فون ترجمانی سروس کا استعمال کرتے ہوئے کر سکتے ہیں۔ NHS24 اکثر آپ کے گھر کے قریب اور ایمرجنسی ڈیپارٹمنٹ جانے کی ضرورت کے بغیر آپ کو صحیح جگہ پر صحیح طبی دیکھ بھال حاصل کرنے میں مدد کرے گا۔ مثال کے طور پر، آپ کو معمولی چوٹ کے کلینک میں بھیجا جا سکتا ہے یا ڈاکٹر کے ساتھ ویڈیو کال کی جا سکتی ہے۔
Hãy đảm bảo bạn nhận được sự chăm sóc phù hợp tại đúng nơi
Chỉ đến Khoa cấp cứu nếu bạn cần chăm sóc khẩn cấp cho các trường hợp khẩn cấp như nghi ngờ đau tim, đột quỵ hoặc chảy máu quá nhiều. Trong trường hợp này, hãy gọi 999 bằng dịch vụ phiên dịch qua điện thoại của chúng tôi.
Nếu bạn đến Khoa cấp cứu với các triệu chứng khác, bạn có thể bị từ chối và chuyển đi nơi khác nếu bạn không ở đúng nơi để được chăm sóc phù hợp. Nếu bạn ở lại, bạn sẽ phải chờ rất lâu vì bất kỳ ai có tình trạng khẩn cấp hơn sẽ luôn được khám trước, ngay cả khi họ đến sau bạn.
Nếu bạn nghĩ rằng mình cần đến Khoa cấp cứu nhưng không nguy hiểm đến tính mạng, hãy gọi NHS24 miễn phí theo số 111.
Bạn có thể làm điều này bằng dịch vụ phiên dịch qua điện thoại của chúng tôi. NHS24 sẽ giúp bạn nhận được dịch vụ chăm sóc y tế phù hợp tại đúng nơi, thường là gần nhà hơn và không cần phải đến Khoa cấp cứu. Ví dụ: bạn có thể được giới thiệu đến phòng khám chấn thương nhẹ hoặc gọi video với bác sĩ.
Lọ si Ẹka Pajawiri nikan ti o ba nilo itọju ni kiakia fun pajawiri gẹgẹbi ikọlu ọkan ti a fura si, ikọlu tabi ẹjẹ ti o pọ ju. Ti eyi ba jẹ ọran, pe 999 nipa lilo iṣẹ itumọ tẹlifoonu wa.
Ti o ba lọ si Ẹka Pajawiri pẹlu awọn aami aisan miiran, o le yipada kuro ki o firanṣẹ si ibomiiran ti o ko ba wa ni aye to tọ lati gba itọju to pe. Ti o ba duro, iwọ yoo duro de igba pipẹ nitori ẹnikẹni ti o ni ipo iyara diẹ yoo ma wa ni akọkọ nigbagbogbo, paapaa ti wọn ba wọle lẹhin rẹ.
Ti o ba ro pe o nilo lati lọ si Ẹka Pajawiri ṣugbọn kii ṣe idẹruba aye pe NHS24 ni ọfẹ lori 111.
O le ṣe eyi nipa lilo iṣẹ itumọ tẹlifoonu wa. NHS24 yoo ṣe iranlọwọ fun ọ lati gba itọju ilera to tọ ni aye to tọ, nigbagbogbo sunmọ ile ati laisi iwulo lati lọ si Ẹka Pajawiri. Fun apẹẹrẹ o le tọka si ile-iwosan ipalara kekere tabi ni ipe fidio pẹlu dokita kan.
NHS Greater Glasgow and Clyde is committed to becoming a leading anti-racism organisation. We want to ensure that our workforce at every level represents the communities we serve and that we are inclusive and welcoming of all patients and staff.
We recognise that racism is a fundamental cause of poor health in affected populations.
We believe our workplace should be a place where discrimination is unacceptable.
We plan to –
actively seek out and remove racism and discriminatory practice
identify the systems and behaviour that are allowing this to happen
ensure that everyone feels able to bring these to light.
Through our tried and tested methods, our staff and patients with lived experience of racism will tell us how well we are doing this. Along with our network of anti-racism organisations, they will also help us shape our ongoing work.
Our actions are grouped under the following themes.
Leadership and Accountability
Our leaders will be visible in their commitment to stand against racism and will work together to ensure their power and influence successfully delivers our goals. They will continue to invest in established anti-racism work, including activity to increase representation of Black and Minority Ethnic (BME) people in leadership positions.
Data and Evidence
Our workforce will be supported to provide equality monitoring data that will allow the organisation to determine whether we have a workforce that reflects the communities we serve. This information will allow us to identify any additional measures that need to be taken to ensure inclusion across all areas.
Patient data will be used to measure whether our services are meeting the needs of BME people. There have been significant improvements in gathering ethnicity data in recent years, however more examination is required to find out if we are consistently providing improved access to services for BME people.
Workforce, Culture and Wellbeing
Our ongoing workforce activities will continue to focus on creating fair opportunities and promoting our anti-racist position. These include a dedicated BME leadership programme and a supported BME Staff Network.
Staff are supported to report perceived Hate Crime incidents via NHSGGC’s incident reporting system. Racist incidents are the most commonly reported, which has led to system-wide campaigns supported by resources and training.
We will deliver equality, diversity and inclusion training to all NHSGGC managers which will highlight the manager’s role in tackling racism in the workplace. This will sit alongside our delivery of a range of anti-racism learning opportunities developed by the Coalition for Racial Equality and Rights (CRER).
Equality Focused Service Delivery
Our Equality Impact Assessment (EQIA) Programme will continue to be used to highlight the impact any service changes may have on particular communities or groups of patients.
A new Frontline Equality Access Tool (FEAT) is now being used in hospital services to better understand how equality law is translated into everyday activity. The tool allows us to identify areas where staff need additional support to ensure they meet the needs of all patients. This work has helped us develop a patient pathway app, ‘Meeting the Needs of BME People’, which supports staff in understanding and responding sensitively to the needs of BME patients.
The Frontline Equality Assessment Tool (FEAT) has been designed to ensure that every service gets it right every time for all our patients.
Developed in response to feedback from our staff on areas where they feel NHSGGC could be doing better, the Tool also takes into account evidence from the experiences of our patients.
The FEAT focusses on assessing how we can fully meet the needs of all our patients within frontline services. It will be used by lead members of local service teams in collaboration with the Equality and Human Rights Team to look at patient flow and integration of inequalities sensitive practice.
This will involve reviewing how patient data is collected, how communication support is assessed, knowledge of protected characteristic-related issues and associated policies and protocols as well as the impact on discharge planning.
By translating the language of legislation into practical steps for staff, the FEAT offers a sense check which highlights both where there are gaps in services’ inequalities sensitive practice and where there are examples of good practice which could be replicated in other services.
William Edwards, Deputy Chief Executive, NHSGGC
“The Frontline Equality Assessment Tool is a great addition to our processes to enable us to understand and meet the needs of our patients with protected characteristics. Not only will it help us identify where we can take positive action but will also capture where good practice is underway and share across all wards and services.”
Alastair Low, Manager, NHSGGC Equality and Human Rights Team
“Equality legislation can sometimes be seen as distinct or detached from the daily interactions that are at the heart of everything we do. We want to help change that perspective. The time we spend visiting departments will strengthen our understanding of equality legislation and its role in delivering effective, efficient and inclusive services.”
Disability Discrimination Audits (DDAs)
NHSGGC has a duty to remove access barriers for disabled patients. This takes the form of Disability Discrimination Audits (DDA) which involve conducting access audits in partnership with disabled people.
In addition to DDA audits, the Frontline Equality Assessment programme also includes a rapid assessment of a physical environment with proposed enhancements reported back to our Estates and Facilities Directorate.
We are currently carrying out a range of DDAs and FEAT reviews in Acute settings which aim to identify any adaptations required.
Professor Tom Steele, Director of Estates and Facilities
“We know that some aspects of the physical environment can still present barriers for some people who use our buildings. We are committed to a programme of ongoing improvement works as well as deigning space that will act as an enabler to staff, patients, carers and visitors.”
This information is for the attention of all NHSGGC staff involved in the treatment and care of Black and Minority Ethnic patients (BME). Following these guidelines will help ensure that our BME patients access the services and treatments that meet their needs. This information is also available on the Right Decisions app.
Around 5% of our BME patients do not speak English. This group of patients have additional barriers to accessing our services that must be addressed.
Getting It Right for BME patients – Core Elements
Expectations for all NHSGGC staff
Treat people fairly – treat BME people fairly and without prejudice or stereotyping. NHSGGC has a zero tolerance policy on discrimination.
Know your community – have knowledge of the local community who may use their service, including an ethnicity and language breakdown.
Collect ethnicity data – always collect the ethnicity of patients using your service. This is mandatory in Scotland for Acute services. TrakCare care and EMIS enable you to record the ethnicity of people who use our services in the demographics pages. People can say ‘prefer not to say’ but we need to ask all people who use our services. Anyone who comes into contact with a patient and has responsibility for checking their demographics to confirm identification and should update their details including ethnicity. Patient demographics which includes ethnicity should be checked on every visit for every patient to a hospital to ensure it is fully updated. If available on paperwork prior to visit e.g. through a GP Referral, then whomever is logging this on the system should update demographics. The patient does not always need to be present for the first update. All patient must have their ethnicity recorded.
Prepare translated resources – have resources about your service ready, including consent to treatment forms, for your BME patients who may not speak English. Have a stock available in the languages you use most and know how to access others when required. For more information go to Clear to All.
Know how to access interpreting support – It is our responsibility to provide interpreting support for any patients using our services. Support is available either via telephone or face to face interpreters. For more information go to Interpreting Services
Ensure patients know how to access interpreting support – patients who don’t speak English can use our telephone interpreting service to call your or any other NHSGGC service. Patient leaflets are available for immediate download in 40 languages. See Direct Patient Access information. Other languages can be provided for your patient.
Get feedback from BME patients – ensure that any patient engagement is inclusive of BME communities, including non-English speakers
Know how to access staff training that covers race equality – you can log in to LearnPro for the statutory and mandatory equality training
Source: Joseph Rowntree Foundation
Know your population
Scotland’s BME population
The 2022 Census has provided evidence of the changing ethnic composition of Scotland.
Of the 5.4 million people living in Scotland, around 388,000 came from Black/Minority Ethnic backgrounds, which equates to around 7% of the total population – a rise of 3% from the 2011 census figures.
Asian groups were the largest minority ethnic group in Scotland and represent nearly 4% of the total population. White minority ethnic groups (e.g. Irish, Gypsy/Traveller, Polish) collectively make up 5.8% of the total population – a rise of 1.6% since the 2011 census.
Scotland’s BME population is patterned by age, with 11.6% of Scotland’s total population being BME people under the age of 18. This compares to just 1.5% of Scotland’s total population being BME people over the age of 65.
Glasgow is the most ethnically diverse place in Scotland with 20% of Glaswegians coming from BME backgrounds. Notably 32.6% of Glasgow’s under 18 year olds come from BME backgrounds.
Community Languages
About 5 in every 100 people admitted to our hospitals as inpatients do not speak English.
NHSGGC has over 100 language groups that use our services. The top 10 languages are currently:
Arabic
Urdu
Polish
Mandarin
Romanian
Farsi
Punjabi
Kurdish Sorani
Cantonese
Slovakian
Your service’s patient population may not reflect these main language groups so it is important to monitor this. For example, a patient population which is mainly drawn from refugees and asylum seekers will have a different language profile.
Engagement
Services need to establish an understanding of needs by engaging with BME patients and staff to identify issues for BME patients in our services. This can include data collection around ethnicity. It is important to note that all of us have an ethnicity and therefore all patients should be asked their ethnicity in our services.
Services should regularly engage with patients to understand what they think about the services we provide. It is important to include BME patient specifically in patient engagement to ensure their voice is heard in how to improve services. Speak to the Board’s Patient Experience and Public Involvement Team (PEPI) for advice.
Taking an anti-racist approach
Taking an anti-racist approach means ensuring that how we behave or design and operate our services does not discriminate against BME people.
Discrimination means treating people less favourably due to their colour, nationality (including citizenship), ethnicity or national origin (Equality Act (2010)). We all have an ethnicity.
As NHSGGC staff we need to recognise that racism – or any form of discrimination – is a fundamental cause of poor health in affected populations.
We need to create an environment free from racism and stereotyping. We have a responsibility to deliver Person and Family Centred Care to all our patients, based on their individual needs and best practice. Do not make assumptions about a patient’s needs – ask them.
It’s important to recognise that being in the majority group brings with it a level of power and belonging that BME people may not attain. Pointing out perceived differences in appearance, describing BME patients as ‘not our patients’ or as ‘foreign’ when they were born here, all contribute to ‘othering.’
This ‘othering’ can often take the form of using offensive language. Sometimes people will describe certain language as ‘banter’ or ‘having a laugh,’ which can make it difficult for someone to challenge. It is important to always speak up and address the use of offensive language that may be heard in our services.
Racism is classed as a Hate Incident or Hate Crime and should be reported through the NHSGGC Datix Incident reporting system
Inclusive Care
Patient Information
Provision of patient information is a key aspect of health services whether this is written, verbal or in other formats.
Services should assess all patient facing written information to ensure it is accessible.
Identify the core information patients will need and have this available in plain English before requesting translations through the Clear to All service. Clinical letters, diagnostic instructions and compliance-related written information specific to an individual patient can also be translated through this service.
Some patients will wish to take home information about their condition in English, as well as the language they read. This is so family members who read only English are aware of the details.
If your service has high numbers of service users who do not speak English, identify the language profile over a few months and decide on an appropriate stock of your core service information in community languages. For example, in the NHSGGC area there are over 100 languages in use. Maternity Services reviewed their language profile and identified that their service information should be translated and made readily available in at least 10 community languages. Any language out with this list could then be requested via Clear to All as required.
Please be aware if your leaflet is providing additional information through links to English language websites. If the information is integral to the content, it should be translated and provided separately. Otherwise, the leaflet should include a statement to say, ‘If you are unable to access the information on this site, please speak to your clinician’.
All patient leaflets should include the NHSGGC statement regarding availability in accessible formats. For more information go to Alternative Format/Language text section at Interpreting & Language Resources.
When you have completed your review of your service leaflets and implemented this approach, ensure that all staff are aware of how and when to use patient information.
Consider, when making new resources, how this will be translated. This particularly relates to audio and video resources. Liaising with Clear to All is essential to establish the most suitable format. Videos can be voiced over (not subtitled) in community languages but ensure the images used in videos represent our diverse population.
Provision of Interpreting Support
It is our responsibility to provide interpreting support for any patients using our services. All staff should therefore have good awareness of and confidence in using the NHSGGC Interpreting Services.
Support is available either via telephone or face to face interpreters. For more information on how and when to use the service, and resources such as, How to Access Interpreting posters, go to Interpreting Services
Patients who don’t speak English can use our telephone interpreting service to call your or any other NHSGGC service. Please ensure that your patients are given an information leaflet explaining this service in the appropriate language. Leaflets are available for immediate download in 40 languages and can be requested if not currently available. See Direct Patient Access information.
If you or your service would like to attend training on how to use interpreting services, go to our training webpage.
Barriers to Accessing Services
Adopting a flexible appointments system will help ensure that non-English speaking patients have the time they need to communicate and understand any exchange. This also applies to anyone who needs additional time to speak or who uses communication support e.g. patients who have a learning disability, speech difference or British Sign Language user.
Cultural and social issues may be an additional barrier to accessing certain services for some BME communities. For example, there is not a specific word that means ‘depression’ in certain languages, including Punjabi, Urdu and Hindi. The stigma or lack of understanding of mental health problems may be a prohibiting factor for some individuals accessing any NHSGGC services. Also, if patients experience negative or racist attitudes from staff, this will prohibit them from engaging effectively with health services.
If there is a NHSGGC registered healthcare chaplain available on site, they can assist in supporting staff and BME patients and if appropriate, can access specific faith leaders that may provide reassurance for some BME patients. Visit our website for more information.
Community isolation may be a barrier for individuals from smaller BME groups or people who have sought asylum. These individuals may have little or no understanding of the availability of services or how they are provided. This can result in isolation from many statutory services, including the wider health services. Issues relating to migration status can exacerbate such problems.
Your service may work with particular voluntary organisations who could help with considering how best to reach and engage with BME communities. Organisations who can support staff include the Integration Networks e.g. Maryhill Integration Networks, Amma Birth Partners, Red Cross for asylum seekers and refugees.
Acute Patient Pathway – Issues to consider
Pre-admission/Admission
Where possible, ensure staff are aware of your patient’s additional support needs and condition history before they attend. SCI gateway referral letters should highlight if an interpreter is required and any other additional needs.
At times, however, this may not be listed on the referral letter.
It is good practice for staff to routinely ask, “Is there anything I need to be aware of when planning your care?” This may include barriers to accessing appointment times, preferred communication methods/support or issues with travel costs.
Ensure that the patient’s interpreter needs are recorded in the ‘demographics’ on TrakCare and not only on an alert. Update TrakCare if you have a patient who does not speak English and you were unaware of this before they attended their appointment.
Use telephone interpreting if a face to face interpreter was not secured, even to just re-appointment and explain what is happening. Telephone interpreting can be used for the majority of NHSGGC appointments.
Patients who require any kind of communication support will need flexibility within their appointment. Please provide this time to ensure that patients using an interpreter fully understand the information being conveyed and have the opportunity to ask any questions. Make sure that what you have said has been understood.
For face to face interpreting support, check if the patient has stated a preference for the interpreter’s sex.
Do not use family members or bilingual staff as interpreters. Do not use Google translate.
More information on NHSGGC’s policy regarding interpreting support can be found in the policy document.
During Stay
BME patients and carers should be supported and empowered to have their say regarding co-produced care and treatment plans.
Understanding the parameters of our services is important to all our patients. Staff should ensure that the patient understands the service or treatment and why they are receiving it to ensure compliance and consent. Checking that this information is fully understood will maximise benefits to the patient.
Do not exclude non-English speaking patients from group work – they should be offered every part of the patient pathway in line with English speaking patients. The Interpreting Service can offer interpreters who are particularly skilled at working in group settings and can advise staff accordingly.
Discharge
Check that your patient fully understands their discharge plan in terms of clinical follow-up, self-care and supports in the community. If interpreting support is required for this, note that this intervention will take a longer time to complete.
It is vital to use interpreting support at the point of dispensing medication to ensure your patient understands the purpose of their medications and when and how to take it.
Information prescriptions have been used to support this in some services, with translations made as required. Ensure your non-English speaking patient knows how to call back to the pharmacy if they have any questions about their medication, using the direct access telephone interpreting service.
BME communities in NHSGGC have high rates of poverty, and many patients can find themselves going home to difficult circumstances. Please use the Money Worries web page to access simple NHSGGC referral pathways to money advice services and interventions such as the Home Energy Crisis Response Service.
Supporting Information
Clear to All – accessible information guidance and support
Meeting the needs of Autistic people and people with other types of neurodivergence
This information is for all staff involved in the treatment and care of Autistic patients and patients with other types of neurodivergence.
Using these guidelines will help ensure that neurodivergent people are enabled to access services and undergo treatments in a manner which fully addresses their needs. This information is also available on the Right Decisions app.
What is Neurodiversity?
Neurodiversity is the term that explains the natural variation in everyone’s brain, including thinking processes, information processing and learning approaches.
We’re all neurodiverse – all our brains are different. However, over 15% of people in the UK, or roughly 1 in 7 individuals, are neurodivergent.
A neurodivergent person’s brain processes information differently from what is considered typical for most people. Autism, attention deficit disorders (ADHD), dyslexia and dyspraxia are some examples of the most widely recognised neurodivergent conditions.
Most neurodivergent conditions are experienced within a spectrum – meaning that the experience will differ from person to person. A person can also identify with more than one type of neurodivergence.
Neurodivergent conditions tend to be invisible, which can create barriers for individuals in accessing the support they may need to thrive in society.
The concept of neurodiversity recognises the value of each variation making up the range of human thinking, whether it be neurotypical or neurodivergent.
It is important to use inclusive language when discussing neurodiversity, and individuals’ personal choices on how they identify should always be respected. However, identity-first language is generally preferred among neurodivergent communities, such as saying ‘autistic people’ rather than ‘people with autism’.
Autism
What is Autism?
“Autism is a lifelong developmental disability which affects how people communicate and interact with the world”.
“Autism is not a disorder… it is a neurological difference: one with a unique way of thinking and experiencing the world.”
These quotes indicate the range of opinion which exists when seeking to define Autism or being Autistic. One firmly describes Autism as a deficit based disability whilst the other considers Autism as part of the broad range of neuro types (Neurodiversity) which exist in the world.
You may often hear the term “Autism Spectrum” which reflects the range of ways someone can experience being Autistic. It is different for everyone. Some people will require very little or no support with their day to day life whilst others may live in a supported environment. Many people will have levels of support somewhere in between and these needs may vary over time.
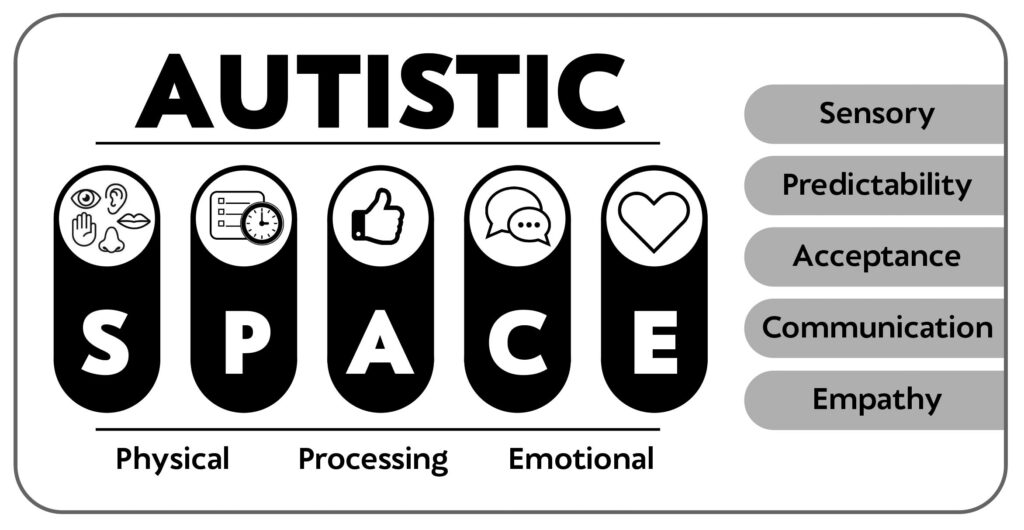
Identifying Needs – the Autistic SPACE Framework
The variability in the experiences of Autistic people can make it difficult to create a standardised approach to patient care. The Autistic SPACE framework has been developed by Autistic Doctors International to encompass the breadth of autistic experience and healthcare access needs.
SPACE Diagram
Sensory needs – Sensory sensitivities are common to almost all Autistic people but the type of and degree to which people experience these varies. Hypo or hyper-reactivity to any sensory stimuli is possible and can vary contextually.
Predictability – Access to healthcare is best maximised for Autistic people when the environment and context is made as known and predictable as possible. Sudden or unplanned change is particularly difficult.
Acceptance – It is important to have a holistic approach, in which Autistic characteristics are understood and accepted.
Communication – Autistic people communicate differently. Many use fluent speech, but may experience challenges with verbal communication at times of stress or sensory overload. Others may be non/minimally speaking and use augmentative and alternative communication methods, including visual cards, writing or electronic devices.
Empathy – Autistic people do not lack empathy but it may be experienced or expressed differently from people who are not Autistic.
Physical, Emotional and Processing Space
Autistic people may need more physical space. Proximity to others, particularly within touching distance, is often difficult to tolerate.
Identifying, processing and managing emotions can be challenging, particularly when Autistic ways of expressing emotions are not understood. Sensory overload or overwhelming emotions may lead to Autistic meltdown or shutdown. Considering this will minimise risks, but if it occurs, the best approach is often to allow space to recover.
Understanding that Autistic people may need additional time to process new information or unexpected changes when compared to non-Autistic people is invaluable in improving the accessibility of healthcare.
Autistic Meltdowns/Shutdowns
A meltdown is an intense response to an overwhelming situation. It happens when someone becomes completely overwhelmed by their situation and can lead to a temporarily loss of control of their behaviour.
Whether in terms of outward expression (meltdown) or inward expression (shutdown), this is often brought about by lack of consideration of the Autistic SPACE principles outlined here.
Neither of these things should be viewed as challenging behaviour but if they do occur the best approach is often to allow space for the person to recover.
Experiencing persistent meltdowns/shutdowns can lead to Autistic burnout, characterised by pervasive, long-term exhaustion, loss of function, and reduced tolerance to stimulus. Application of the Autistic SPACE principles can help go some way to reducing this. For further information and advice on Autistic meltdowns, see the National Autistic Society website.
Other types of neurodivergence
Attention Deficit Hyperactivity Disorder (ADHD):
Refers to a group of behavioural symptoms which include difficulty concentrating and paying attention, hyperactivity and impulsiveness
Dyslexia
Difficulties in learning to read, write and/or spell, including reading and writing. A Dyslexic person can also have associated problems such as remembering and processing information.
Dyspraxia – Also known as Developmental Coordination Disorder (DCD).
Affects physical coordination and balance.
Can also affect working memory and cause difficulties of organisation and planning
Dyscalculia
Makes it difficult to understand and work with numbers, perform calculations, and remember mathematical facts.
Addressing barriers
Research tells us that a range of barriers to accessing and receiving health services exist for neurodivergent people.
These will vary from person to person, so it is important to have open communication to ensure that you understand what the issues may be and how best to address them.
Examples could be –
Staff not understanding condition
Find out about the person’s condition and how it affects them. Gain better knowledge through training opportunities.
Not feeling listened to
Give the time necessary to listen to the person’s experience and clarify any information given.
Use advocates where necessary.
Uncertainty/anxiety
Provide clear information about what to expect. Provide the opportunity for the person to ask questions ahead of particular appointments.
Difficulties with concentration
Too much information and complex language causes issues for most patients. Ensure your information is provided in stages, is clear and simple and is being understood at each point of delivery.
Many of the adjustments that should be considered at each part of the patient’s journey will apply to patients with other types of neurodivergence. See the Autism Acute Patient Pathway for more detailed examples.
Acute Patient Pathway
Issues to consider
This pathway focuses on measures that should be considered at each part of the patient journey to address possible barriers and concerns for Autistic people.
Many of these issues will apply to patients with other types of neurodivergence. Each person’s experience will be different – it is therefore important to communicate with patients to learn their individual needs.
Pre-admission
Give as clear a picture as possible of what the person can expect to happen.
Information (in appropriate formats) should include an explanation of processes and medical terminology. It should also, where possible, include routes to buildings/clinics from point of arrival at the hospital.
If there is sufficient advance notice of the admission, offer the opportunity for a pre visit or additional information to reduce anxiety levels about the experience. This will also aid staff understanding of what is required to improve a patient’s journey.
If it is an outpatient appointment, try to give an Autistic person appointments at less busy times of day. This may help reduce stress levels caused by busy environments.
Admission
Is the reception desk in a noisy or brightly lit area? Is there a lot of information for the Autistic person to process? Consider using a quieter, less brightly lit space for admission and allow time for the person to ask questions and process what they are being told.
If there has been no opportunity to chat or answer questions prior to admission, staff should take extra time to ensure the Autistic person (and where relevant their family/carer/partner) has understood what is happening. Speak clearly, giving the Autistic person time to process the information. If someone is non-verbal do not assume that they do not understand what is being said.
During Stay
If the waiting area is brightly lit or noisy consider the use of a quieter, less brightly lit space. Also take into account any smells; is it possible to minimise this?
Consider where the Autistic person will be during their stay in terms of lights, sounds and smells. If necessary try to allocate a quieter less brightly lit space away from strong smells.
Explain any examinations or processes to be undertaken during the stay. If an Autistic Person has a carer, enlist their support but do not talk over the Autistic Person.
Any changes which need to be made should be clearly explained to the person as soon as possible. This will give time to enable an Autistic person to process the changes and feel more comfortable.
If it is not possible to find an alternative space, consider what can be done to lessen the environment and sensory influences. A single room can be easier in terms of lessening light, sound and smell. Encourage use of noise cancelling earphones or ear buds. – Many Autistic people will have these but may not be sure of using them in the environment; consider providing such equipment. Some Autistic people also wear dark glasses to lessen the impact of bright light.
Ensure that the Autistic Person is aware of the position of other relevant facilities such as toilets (Accessible toilets if necessary).
Over-stimulation of an Autistic Person’s senses may lead to “stimming”. Stimming is a self-regulatory behaviour intended to soothe or steady an Autistic Person. This can take many forms including humming, rocking and hand-wringing or flapping but will vary from Autistic person to Autistic person. It may also involve the use of stimming tools (sometimes called stim toys) such as fidget spinners or rings and squishy toys or just something the person finds comforting. Not all Autistic people visibly stim and it may go unnoticed by others if it takes a less visible form.
Be aware that a previously vocal person can also shut down when under stress, becoming less able to communicate.
Discharge
When the appointment or hospital stay is over, be clear about what will happen next, including any timescales and the need for follow up.
Take time to go through any information that an Autistic person may need and ensure that it is in a format which is suitable for them. Go through the information with the person if necessary, ensuring you check their understanding. Take special care to ensure any medical terminology is explained.
Good Practice example – RAH Day Surgery
Autistic patients can enter the unit via an alternative entrance which enables a less stressful start to their appointment/stay.
Within their six bedded wards, staff at can pull their dark curtains around individual beds to create more privacy and lessen sensory input. They can also reduce lighting in the individual areas.
Meeting the needs of people with Learning Disabilities
This information is for all staff involved in the treatment and care of people with Learning Disabilities.
Using these guidelines will help ensure that people with learning disabilities are enabled to access services and undergo treatments in a manner which fully addresses their needs.
Learning Disability & Health
A learning disability is a significant, lifelong, condition that starts before adulthood. It affects a person’s development and means they may need help to –
understand information
learn skills
cope independently.
Learning difficulties, such as dyslexia, ADHD, dyspraxia and speech & language issues are not defined as a learning disability.
Within Greater Glasgow & Clyde there are over 6000 adults who have some form of learning disability.
They experience some of the poorest health outcomes of any group in Scotland and much of their health needs are unrecognised and unmet.
People with learning disabilities also have a different pattern of health needs. They also die younger and have differing causes of death from the general population, often from preventable causes.
People with a learning disability are –
living with, on average, 5 long term health conditions compared with 1 or 2 in the general population
more likely to have mental health problems – 40-50% compared to 1-10% of general population
more likely to have a sensory impairment – approximately 60% will have a visual impairment and 40% will have a hearing impairment
more likely to be underweight or obese than the general population.
People with learning disabilities experience a number of barriers when trying to access appropriate healthcare within the NHS.
Patients often lack confidence and do not understand the information they need to make informed decisions about their health needs or about their treatment.
There is often insufficient joint working from different care providers, aftercare/follow-up care and carer involvement.
Acute Patient Pathway
Pre admission/appointment
Consider contacting the local LD Nurse Team and find out if they can provide additional support or advice for staff.
Provide the patient with full clear information about their hospital visit/ appointment.
All information should be provided in an appropriate format – this may be easy-read/ words and pictures format. To request translation of information into easy read or any other format, contact cleartoall@ggc.scot.nhs.uk
All information should include an explanation of processes and medical terminology. Explain clearly what the patient can expect to happen during their appointment or hospital stay. It should also, where possible, include routes to buildings/clinics from point of arrival at the hospital. If there is sufficient advance notice of the admission, offer the opportunity for a pre visit or additional information to reduce anxiety levels about the experience. This will also aid staff understanding of what is required to improve a patient’s journey.
If it is an outpatient appointment, try to give the patient an appointment for late morning or early afternoon. Many people with a learning disability may take longer to get ready and leave the house in the morning. This is particularly true for people who have additional support needs and are supported by a carer.
As soon as possible, staff should find out the capacity status of the patient and, if applicable, ensure legal guardians are consulted in treatment consultations. Patients may also require a Section 47 Certificate of Incapacity.
Admission for inpatient or day procedure
Prior to admission, staff should find out the capacity status of the patient and, if applicable, ensure legal guardians are consulted in treatment consultations. Patients may also require a Section 47 Certificate of Incapacity.
When the patient comes in, ask them if they have all of the support they need. If required give further information or support regarding what is going to be happening during the appointment.
If there has been no opportunity to chat or answer questions prior to admission, staff should take extra time to ensure the patient (and where relevant their family/carer/partner) has understood what is happening. Speak clearly, giving the patient time to process the information. If someone is non-verbal do not assume that they do not understand what is being said.
During outpatient appointment or day surgery
Prior to admission, staff should find out the capacity status of the patient and, if applicable, ensure legal guardians are consulted in treatment consultations. Patients may also require a Section 47 Certificate of Incapacity
Explain any examinations or processes to be undertaken during the stay. If the patient has a carer with them, find out how they might be able to provide support during this conversation.
Any changes which need to be made should be clearly explained to the person as soon as possible. This will give time for the patient to process the changes and feel more comfortable.
Ensure that the patient is aware of the position of other relevant facilities such as toilets (Accessible toilets if necessary).
During ward stay
When the patient is admitted, make sure that the What Matters to Me board or form is completed. Where appropriate, involve carers and family.
Find out what the patient’s support needs are during meal times and when being given medication. Again, carers/ family should be involved as much as appropriate.
Ensure that the patient is aware of the position of other relevant facilities such as toilets (Accessible toilets if necessary).
Support prior to operation/ procedure – make sure that the patient is fully aware and understands what will happen during pre-surgery and any procedures involved in surgery and in recovery.
As soon as possible, staff should find out the capacity status of the patient and, if applicable, ensure legal guardians are consulted in treatment consultations. Patients may also require a Section 47 Certificate of Incapacity.
Consider contacting the local LD Nurse Team and find out if they can provide additional support for the patient and for staff. LD nurses can advise acute staff on the most appropriate ways to support patients during hospital stay.
Discharge/follow up
Before starting discharge process, make sure the patient has all the support they need to fully participate. If relevant, what role can the carer play during this conversation.
Consider if the patient is already supported by community LD Nurse service. If not, could a referral or link be made on behalf of the patient? How can an LD Nurse provide support during this stage of patient’s care?
Take time to go through any information that the patient may need and ensure that it is in a format which is suitable for them. Go through the information with the person if necessary, ensuring you check their understanding. Take special care to ensure any medical terminology is explained.
Speak with the patient and carer to identify ways in which carers could be involved during aftercare
7 Steps to Equal Healthcare
I am your patient…
Imagine being me
Listen to me
Find out who and what matters to me
If you are not sure what my support needs are or the best way to give me that support, ask me
Give me the information I need in the way that I need it
If necessary, work with others who are involved in my care
Think giving me the treatment and support I need is too difficult? Think again.
Having a supportive conversation with a patient
When speaking with the patient:
If the patient has a carer or support with them, find out how much the patient wants or needs them to be involved.
Speak to the patient directly, not the carer.
At the start, explain what it is you are going to be talking about.
Go at the patient’s own speed and allow extra time for them to process the information.
Use simple language and short sentences: only one idea, question or instruction at a time.
Make sure that patient is following and that they understand what you are telling them. If they are unsure, try a different way of explaining. Is there a way that their carer could help?
Ask if they need you to go over anything again.
When the patient wants to tell you something or to ask questions:
Always allow the patient time to say what they want to say and don’t try to finish their sentences.
You can double check with the patient to make sure that you are clear about what it is they have said or what they have asked.
If you need to examine the patient or carry out any kind of procedure:
Always explain what you are going to be doing before you start.
Support Services
NHSGGC Clear to All
If you are giving the patient any written information about your service or about their health needs, including medication, it is their right to have this in a format that suits their needs. To request translation of information into easy read or any other format, contact cleartoall@ggc.scot.nhs.uk
VIAS is a third sector organisation providing training and consultancy, campaigning and conducting research into what does and doesn’t work in the lives of people with learning difficulties and individuals on the autistic spectrum.
PAMIS works across Scotland supporting people with profound and multiple learning disabilities and their families. This service provides partnership working with families, carers and professionals.
People First (Scotland) works for the human rights of people who have a Learning Disability, offering individual support, training and campaign working.
The Scottish Consortium for Learning Disability (SCLD) is a consortium of partner organisations in Scotland who work together to encourage best practice in the support of people with learning disabilities through training information research and public education; works alongside people with learning disabilities and family carers
SLDO is based within the Institute for Health and Wellbeing at the University of Glasgow. Their aim is to help build a better understanding of the health and health inequalities experienced by people with learning disabilities in Scotland.
Mencap is a UK wide support service that provides personalised support to people and their families and is a leading research and campaign provider on improving the lives of people with a learning disability.
We use cookies to analyse traffic to our site and to enable certain functions such as forms and YouTube videos. These do not collect personal information. By clicking "Accept All", you consent to our use of cookies, or you can customise the options.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
CloudFlare provides web performance and security solutions, enhancing site speed and protecting against threats.
Sequence rules uses cookies to track the order of requests a user has made and the time between requests and makes them available via Cloudflare Rules. This allows you to write rules that match valid or invalid sequences. The specific cookies used to validate sequences are called sequence cookies.
session
cf_ob_info
The cf_ob_info cookie provides information on: The HTTP Status Code returned by the origin web server. The Ray ID of the original failed request. The data center serving the traffic
session
cf_chl_rc_m
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
__cfruid
Used by the content network, Cloudflare, to identify trusted web traffic.
session
__cf_bm
Cloudflare's bot products identify and mitigate automated traffic to protect your site from bad bots. Cloudflare places the __cf_bm cookie on End User devices that access Customer sites that are protected by Bot Management or Bot Fight Mode. The __cf_bm cookie is necessary for the proper functioning of these bot solutions.
session
__cflb
When enabling session affinity with Cloudflare Load Balancer, Cloudflare sets a __cflb cookie with a unique value on the first response to the requesting client. Cloudflare routes future requests to the same origin, optimizing network resource usage. In the event of a failover, Cloudflare sets a new __cflb cookie to direct future requests to the failover pool.
session
_cfuvid
The _cfuvid cookie is only set when a site uses this option in a Rate Limiting Rule, and is only used to allow the Cloudflare WAF to distinguish individual users who share the same IP address.
session
cf_clearance
Whether a CAPTCHA or Javascript challenge has been solved.
session
cf_use_ob
The cf_use_ob cookie informs Cloudflare to fetch the requested resource from the Always Online cache on the designated port. Applicable values are: 0, 80, and 443. The cf_ob_info and cf_use_ob cookies are persistent cookies that expire after 30 seconds.
session
__cfwaitingroom
The __cfwaitingroom cookie is only used to track visitors that access a waiting room enabled host and path combination for a zone. Visitors using a browser that does not accept cookies cannot visit the host and path combination while the waiting room is active.
session
cf_chl_rc_i
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
cf_chl_rc_ni
These cookies are for internal use which allows Cloudflare to identify production issues on clients.