There is a free patient car park at Lightburn Hospital.
Was this helpful?
Yes
No
Thanks for your feedback!
Here are some Success Stories from SWMS service users:
Brian
Brian’s Journey
Brian was referred by his GP to SWMS. He wanted to improve his general mobility and health.
“I needed to ask for help as I knew I couldn’t do it on my own”.
Following his initial assessment, Brian was offered a SWMS Physiotherapy assessment. Brian was struggling with painful joints and was inactive.
“Everything was sore bar my hair”
Brian was provided with a walking stick, walking programme and started the “Get Started” weight management activity classes.
“The classes were good fun and gave me structure to my activity”.
Brian started a SWMS group in February 2019 until March 2020. During this time Brian lost 37kgs (20% of his body weight). Using dietary and activity lifestyle changes. What a fantastic achievement!
The SWMS staff helped me to change my lifestyle without being judgemental.
“The group support was really helpful. Everyone was on the same journey which made the process easier”.
Catherine
Catherine’s Journey
After years of yo yo dieting, I was referred to SWMS in June 2019, weighing 152kgs. My aim was to lose weight, to reduce my significant joint pain, and ultimately improve my low mood.
Following my initial assessment, I was referred to the Psychology team, where I discussed my issues with eating control and anxiety. I was given techniques to support my issues and was offered a special “disordered eating” group programme.
The “COVID-19 lockdown” interrupted my treatment. I now attend my disordered eating group and Psychology sessions via a video appointment, which has worked well for me.
The team physiotherapist has helped me become more active and I follow the SWMS exercise video regularly.
“!I’ve had many failed attempts but I do think having Cognitive Behavioural Therapy really helped, plus being more realistic – it’s not a quick fix – it takes time, planning and organisation. Realising that going off track is not a failure. It’s being kind to yourself and continuing with the plan. Tracking is my saviour. You have to know what you are eating. Every time I’ve lost weight it’s because I knew what was going in. It’s very easy to lose track with mindless eating”.
Susan
Susan’s Journey
I came to SWMS after years of weight loss success and failures. I am now in my second episode of care building on previous learning.
“The team have an enormous amount of clinical expertise, who don’t quit and stay cheerful – it’s catching!”
Following my first assessment in the service I lost 34.5kgs. I engaged in the lifestyle programme and attended SWMS moderate intensity exercise classes and Physiotherapy – as even sitting around gets hard after a while.
I relapsed, regaining weight having to tackle my depression and binge eating behaviours: The Psychologists in the service helped me focus on the cycle of change in accepting and refocusing in periods of weight regain through Cognitive Behavioural Therapy and Mindfulness in group sessions and 1:1 therapy.
In the midst of COVID-19 I am now receiving Interpersonal Psychotherapy with a SWMS Psychologist through telephone consultations. I am now at my lowest weight in the service and in many years.
“To make change you have to believe in the possibility of change and this is what the SWMS has helped me so much with. I have had weight loss successes and failures and have been able to deal with whatever has happened”.
Was this helpful?
Yes
No
Thanks for your feedback!
Public Health Directorate
This section provides information on Public Health issues and functions. Much of the information will be of interest to staff and professional audiences working in the fields of Public Health and health improvement.
Influence policy and strategy including legal and fiscal measures to protect and promote health and reduce health inequalities.
Work with communities and partner organisations to improve health and reduce inequalities
Provide leadership for Public Health across NHSGGC and partner organisations
Ensure the protection of the public from communicable and non-communicable diseases and environmental hazards
Monitor the pattern of disease in the community
Assess the health needs of the population and advise how these needs can be met
Facilitate the strategic development of health care services provided
Ensure the systematic implementation of evidence based practice, clinical and quality standards for healthcare, preventative programmes and interventions such as screening; immunisation and behaviour change
Provide support for professional development – building capacity, research and evaluation services, access to evidence base and services to ensure dissemination of resources.
On 21st August 2018 NHS Greater Glasgow and Clyde Board approved “Turning the tide through prevention“, our new ten year Public Health Strategy.
Our vision is to improve our population’s health and tackle health inequality.
We will build on our relationships with staff and residents across NHSGGC to adopt healthier lifestyles by working with, and supporting local communities, employers and staff. To deliver our vision, our mission is to focus on the changeable determinants of ill health and provide clarity and co-ordinate efforts to prevent health inequalities and to enable our staff and partners to deliver our vision.
Our Public Health Challenge
High numbers of children and families who continue to experience poor outcomes
Increasing number of individuals and families affected by poverty, debt, fuel and /or food poverty and homelessness
Poor life expectancy, high levels of morbidity and disability and the need to access a wider range of health (and other) services at a younger age and for longer than other areas of Scotland
Appropriately meeting the needs of an increasingly ethnically and culturally diverse population and delivering accessible, needs based services
High demand on resources associated with mitigating the impact of health inequalities on individuals rather than influencing their prevention upstream.
Priorities for preventing ill-health and early intervention
These include:
Improve identification and support to vulnerable children and families
Enable disadvantaged groups to use services in a way which reflects their needs
Increase identification of and reduce key risk factors including those associated health inequalities (smoking, healthy weight, drug, alcohol use and poverty mitigation)
Promote mental well-being, reduce disabling distress and suicide and ensure early intervention for mental ill health
Embed the principles of the health promoting health service across care settings
Increase the use of anticipatory care planning; vaccinations and screening
Increase the proportion of key conditions including cancer and dementia detected at an early stage
If you need to contact us for any reason, please phone 0800 592087 or email us on appointmentsbookingcentre@ggc.scot.nhs.uk. This is open Monday to Friday 8.00am – 8.00pm and on a Saturday 9.00am – 1.00pm (excluding Public holidays). 5pm – 8pm tend to be the quieter times to contact by phone.
When you contact the booking centre, please give a short description of what you need, e.g. a repair, review, new assessment or advice. This will be recorded as a new referral. Do not worry if the booking centre staff say you have been discharged, you can self-refer at any time. You can book a review appointment within 12 weeks. If it’s been longer than this, you will be asked to make a new appointment.
An experienced Orthotist looks at all the referrals, They might phone you to talk about your referral or may add you to the right waiting list without needing to speak to you. You will then get a text message or letter asking you to book an appointment.
You can also manage your Orthotic appointments through the Patient Hub online portal. Patient Hub is an online portal providing you with information relating to your care, all at the click of a button. It can be accessed securely using a smartphone, tablet or computer. You can log in to patient hub here.
We offer virtual appointments which are video appointments via NearMe. Do not worry if you cannot do video calls, the Orthotist will phone you.
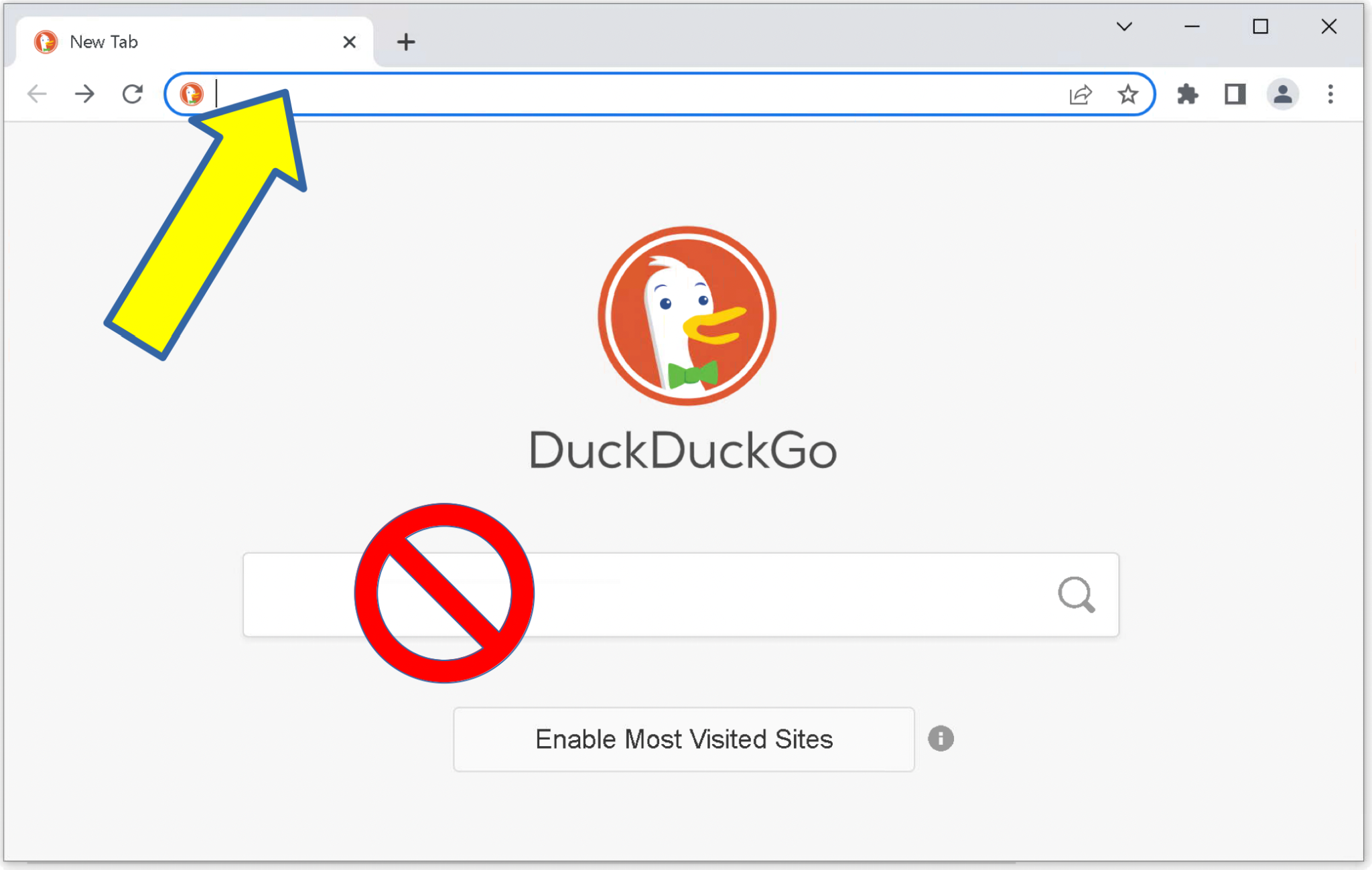
Top tip: To make sure you are in the correct waiting area, use the full URL rather than a search engine, as this can lead to a different waiting area being presented as the top result.
What is Near Me?
Near Me is a video consulting service that enables people to have health and social care appointments from home or wherever is convenient. All you need is a device for making video calls like a smartphone and an internet connection. Near Me is a secure form of video consulting approved for use by the Scottish Government and NHS Scotland.
How does Near Me work?
We will send an Orthotic appointment letter with a date and time, including the website address and a link for the video clinic. However, there is no need to download an App or create an account, or provide personal details such as passwords or pin numbers. We will ask the same questions if you were face to face in the clinic.
Occasionally, Near Me video consulting is not suitable for all consultations, for example, if you need a physical examination or a procedure. The orthotist can advise you on what is appropriate for you. We will send a leaflet that gives you support to get set up and start your call.
You will see either a qualified Orthotist, student Orthotist (under supervision) or an Orthotic clinical assistant practitioner. We will ask questions about your problem. Everything you tell us is confidential. The physical assessment may involve the Orthotist touching the affected area, testing your movement and strength and assessing your mobility.
After your assessment, we will discuss your problem; agree goals and a treatment plan with you. We can also offer advice and exercises to allow you to manage your problem yourself.
The treatment plan may include a customised or custom made orthotic device. In order to make a device to fit you, we may need to take measurements, scans or casts.
Emergency slots are kept for patients where they do not have a spare orthosis to use while awaiting repairs. Technicians in the Orthotic Workshop in Gartnavel General Hospital can carry out emergency repairs on orthoses such as new straps/padding.
A patient or friend, carer or family member can arrange this by asking for an emergency repair when contacting for an appointment. You will not see an Orthotist at these appointments.
Was this helpful?
Yes
No
Thanks for your feedback!
Specialist Children’s Services (SCS) support the health and wellbeing of children and young people across Greater Glasgow and Clyde. We offer a range of services within Specialist Community Paediatric Teams (SCPT), Child and Adolescent Mental Health Services (CAMHS) and Neurodevelopmental Teams.
Most children and young people’s health and wellbeing can be managed by their families and the teams around them such as their health visitor, GP or nursery/school staff. Some children and young people require more support. This support could be provided by SCS. Depending on their needs; children, young people and their families will be supported by the team that is right for them. The team will work in partnership with the child or young person, their family and other services in the child or young person’s life.
Each team is made up of different health professionals including Dietitians, Family and Systemic Psychotherapists, Nurses, Occupational Therapists, Paediatricians, Physiotherapists, Psychiatrists, Psychologists, Speech and Language Therapists and others as needed. Children and young people can be seen by one of these professionals or by a number of them depending on what they need. Most of our services are delivered in the community where children and young people live. Some of our services are delivered through the Royal Hospital for Children (Glasgow) and other sites within NHSGGC.
For more information have a look at Our Services page on the KIDS for Families website and app.
Child and Adolescent Mental Health Services
The Child and Adolescent Mental Health Service (CAMHS) provides community-based and inpatient support to children and young people in NHS Greater Glasgow and Clyde who have significant difficulties with their mental health and wellbeing. These difficulties will be significantly affecting their daily life, getting in the way of going to school, doing their activities or socialising, or puts them at risk of harming themselves or others.
Adolescent Inpatient Unit at Skye House
Skye House first opened on 25th February 2009. It is a purpose-built facility on the Stobhill Hospital site for young people aged 12 to 18 years from across the West of Scotland. Skye House provides a range of dedicated services for young people who are experiencing thoughts and feelings which make it difficult to cope with everyday life. Skye House is a 24-bedded unit.
Mental health services for young people are planned on a regional basis by the West of Scotland NHS Boards (NHS Ayrshire and Arran, NHS Dumfries and Galloway, NHS Forth Valley, NHSGGC and NHS Lanarkshire). Skye House is funded by all these NHS Boards to deliver a service to young people from each area.
The service provides inpatient treatment for young people with conditions like severe depression, eating disorders, psychosis and obsessive-compulsive disorders. Young people may also be experiencing a period of distress whereby they may be safer in an in-patient environment. Length of stay is individual and will always be determined by the best interest of the young person.
At Skye House, we are more than aware of how worried families and young people may be about their admission and subsequent stay. We want you to be reassured that our aim is to work with you collaboratively and our communication and practice is driven by compassionate and individually focused care.
Skye House Adolescent Unit is part of Stobhill Hospital and is made up of three separate buildings:
Therapies Block – Main reception, Staff offices, Group rooms, Therapeutic Kitchen and a Music Room.
Accommodation Block – contains the 3 wings (Mull, Harris and Lewis). There are 8 en-suite bedrooms in each wing. There is also a TV lounge in each wing and there are two dining rooms where all meals and snacks are eaten.
School Block – there are 4 classrooms and a Gym, where young people attend a range of school classes. The Gym can also be used in the evening exclusively by Skye House patients.
We have access to outdoor space. We continue to work to make our outdoor space useable for everyone in a range of ways.
Young people will be admitted to one of the wings. Sometimes they may move to another wing for a variety of circumstances. This will always be discussed with you and your family.
Young people in Skye House are allocated a Psychiatrist, a Named Nurse and an Associate Nurse who will be responsible for the day to day care. You might also work with other colleagues including psychologists, speech and language therapists, dieticians and occupational therapists.
It would always be our intention to admit young people under the age of 18 years to an age-appropriate environment. Very occasionally if a bed is not immediately available and a young person is not safe with community CAMHS support they may need to be admitted into an adult ward. Please be reassured that if this should happen, we will involve you and it will be for as short a time as possible. When on an adult ward young people are supported with age-appropriate activities, remain supervised depending on their care plan and we ensure they are comfortable and safe in this environment. However, on some occasions, this is not possible.
Clinical Psychology – Maternity and Neonatal Psychological Intervention (MNPI) Service
Maternity and Neonatal Psychological Intervention (MNPI) Service operates between three acute based sites:
Queen Elizabeth University Hospital (QEUH)
Royal Alexandria Hospital (RAH)
Princess Royal Maternity Hospital (PRMH)
Hospitals are supported by Clinical and Business Support Staff.
Royal Hospital for Children Govan Glasgow G51 4TF
This service offers antenatal and postnatal psychological assessment and intervention on an in-patient and out-patient basis for abnormal pregnancy and birth, including but not limited to:
Foetal abnormality
Traumatic birth
Premature birth/congenital birth problem(s)
Recurrent loss
Neonatal death
Antenatal anxiety/low mood
Community Child and Adolescent Mental Health Services
CAMHS are teams of professionals who support children and young people (up to 18 years old) experiencing ‘moderate to severe’ mental health difficulties. These are difficulties that significantly affect their daily life. These difficulties get in the way of going to school, doing their activities or socialising, or puts them at risk of harming themselves or others. Lots of children and young people referred to CAMHS have already tried other support.
CAMHS work in partnership with children, young people and their families or carers. CAMHS often work together with other services in the child or young person’s life such as their school. Most CAMHS support is provided in community settings. Although some CAMHS teams are based in hospitals. You can find out more about CAMHS services on the Children and Young People’s page in MyApp: My Mental Health which has been developed for young people in NHSGGC.
Wee Minds Matter is an infant mental health service. We support babies and their families from pregnancy through to the end of the first three years.
Infant mental health is a baby’s developing capacity to communicate and regulate their emotions, form close and intimate relationships, to be able to explore their environment and learn. This all takes place in the context of the first early relationships with parents/primary caregivers.
Supporting the Perinatal and Infant Mental Health Universal Pathway
We recognise that essential valuable work is already taking place with babies and their families across Glasgow and Clyde through the universal pathway within Health, Social care and valuable third sector services.
The Wee minds matter service does not wish to duplicate this work. Instead, we aim to strengthen the capacity of the existing pathway by supporting the existing network. This may be through offering consultation; reflective practice; exploring opportunities for joint working; raising awareness sessions on specific topics; contributing to developing aspects of the pathway e.g. antenatal; and by offering a daily duty line for health professionals for support in thinking about a particular baby and their family, and discussing potential future referrals.
We will work directly with families once all support within the pathway has been exhausted and/or when specialist direct intervention is indicated through joint assessment with referrers and the family and where there are persistent and ongoing concerns for a baby and the parent infant relationship.
Service Offered
Consultation
This will be offered when referrers have a dilemma/question or are concerned about a lack of change in the work with a baby and their family. A consultation will offer a space for joint thinking, within the context of GIRFEC. Clear outcomes will be identified as a result. Consent is always required from the family for this to take place.
Care Planning
Following any request for help we will discuss the current care plan with the referrer, and identify what interventions and support have already been explored and tried, including outcomes. We will think carefully with the team around the baby about the level and type of support needed for the baby and family. During pregnancy, an anticipatory care plan will be prepared to take into account planning for the emotional needs of the baby post-birth.
We aim to ensure that the experience and voice of the baby are adequately and proportionately included within any care plan.
Direct Clinical Work
Direct clinical work will include a range of specialist interventions including speech and language therapy, occupational therapy, Newborn Behavioural Observation (NBO), infant observation, enhanced Solihull approach, Parent infant psychotherapy, art-based group work, circle of security (individual or group), parent-infant support sessions.
Request for Help
If you have concerns about a baby or a parent/infant relationship and require specialist support or would like to discuss a potential referral, please ring our duty line on 0141 201 0808 from Monday to Friday at 9 am – 5 pm.
The service actively encourages early referrals during pregnancy and the first 6 months of an infant’s life as this is an optimal time for growth. However, we will consider all requests for any child under 3 years of age.
We are the Intensive Child and Adolescent Mental Health Services (ICAMHS). ICAMHS are a team of mental health nurses and healthcare support workers.
We are available 365 days a year including holiday periods. We are contactable from 8:00 am till 8:15 pm daily.
What do we do?
We provide intensive treatments both at home and in the community to young people living in Greater Glasgow and Clyde. We can see people at home, school or where feels most comfortable. Our aim is to provide support to young people and their families’ in the least restrictive way.
We are normally involved for a short period of time, we may see a young person for around 6 weeks on average however this time period may be reduced or extended depending on the young person’s needs.
Who do we see and why?
ICAMHS will work with young people under 18 years old who need additional support with their health mental and/or young people with moderate to severe mental health disorders.
Some of the young people we see are living with low mood, suicidality, complex trauma, anxiety, self-harm and eating disorders.
We also work with young people living with psychiatric conditions such as obsessive compulsive disorder (OCD). We offer support to young people and their families who are experiencing co morbid mental health difficulties alongside neuro developmental conditions
What can we offer?
ICAMHS offer a variety of different mental health supports. This can include learning techniques to help manage distress and understand emotions and feelings. Our support is provided alongside Tier 3 CAMHS who will see you weekly whilst ICAMHS are involved.
We provide meal time support (MTS) for young people experiencing eating difficulties such as Anorexia Nervosa.
We work with young people who self-harm also those who have expressed suicidality. Our role is to assess suicidality and manage risk and safety plan with those who experience thoughts of suicide. We work alongside young people in the community to reduce their self-harming behaviour.
Sometimes young people may need to be admitted to hospital due to their mental health difficulties. Our aim is to support young people and their families in the community for as long as is appropriate. We also support young people returning home after a hospital admission.
ICAMHS have a Community Link Worker who covers the Glasgow City Area only. This service offers additional social support to young people and their families who have experienced mental health problems.
ICAMHS presently offer Intensive Psycho Therapeutic Adolescent Suicide Crisis Intervention (IPT-A-SCI). This is a six week programme on offer to young people who are not presently known or involved with CAMHS.
How do you make a referral?
Requests for Involvement to ICAMHS will be accepted from:
All Child and Adolescent Mental Health Services (CAMHS) within NHSGGC
All Child and Adolescent in patient units
Unscheduled CAMHS (UCAMHS)
Out of Hours on call Consultant/Higher Trainees.
Criteria for ICAMHS referrals include:
Under 18 years of age
Resident within NHSGGC
Under the weekly care of Tier 3 or 4 CAMHS
Assessed and discharged by UCAMHS and not known to Tier 3 or 4 CAMHS (IPT AC A Stream)
Presents risk to self or others in context of significant mental health concerns which require intensive supports
Meal Time Support (pertinent to formulation) following screening by Connect ED/CAMHS.
National Child Psychiatry In-patient Unit – Ward 4
The National Child Psychiatry Inpatient Unit, located in Ward 4 at the Glasgow Royal Hospital for Children, provides flexible in-patient psychiatric services for children aged 5-11 years with severe psychiatric disorders, which may be complicated by neurodevelopmental disorders, physical health problems and complex psychosocial factors, requiring the specialist assessment and treatment skills of the multi-disciplinary Child Psychiatry Team based in the Unit. As the unit is a national service we consider referrals from all Scottish Health Boards.
Who Are We
Our team is a well established, highly experienced and a dedicated multidisciplinary team. The team comprises of child and adolescent psychiatrists, mental health nurses, clinical psychologists, a Speech and Language Therapist, occupational therapists, a Mental Health Staff Grade Paediatrician, a Family & Systemic Therapist, an Art Therapist and Administrative Staff. The In-patient Team has a close relationship with paediatric services within the children’s hospital. The team also has close links with a range of other community-based professionals and agencies.
What We Offer
Our team is dedicated to providing care, treatment and support for children under 12 years of age, who are experiencing severe and complex mental disorders leading to significant impairment and/or risk, which cannot be adequately treated within the locality of the Child and Adolescent Mental Health Services (CAMHS). We offer:
In-patient admission for a comprehensive mental health assessment. This may include neuro-developmental assessment bespoke individual and family assessment and therapeutic intervention, as well as advice on further management.
In-patient admission for a closely supervised medication review. This is particularly when outpatient monitoring is deemed unsafe or insufficient.
Consultation to professionals via interagency meetings on complex clinical problems with children who are not necessarily referred for admission.
Teaching and Training
Research and Audit
Referral Process
Referrals are accepted from Child and Adolescent Psychiatrists working within Community CAMHS Teams. In the first instance, the referring clinician should contact the ward and discuss the case with a senior member of staff who may request that a Referral Form is completed for further information. The patient will then be discussed by the Senior Referrals Team and the outcome discussed with the referrer by telephone.
Contact the National Child Psychiatry In-patient Unit
National Child Psychiatry In-patient Unit Ward 4 Royal Hospital for Children 1345 Govan Road Glasgow G51 4TF
Welcome to the Paediatric Clinical Psychology Service at the Royal Hospital for Children (RHC) in Glasgow. We are a team made up mainly of Clinical Psychologists who provide assessments and interventions to children and young people up to the age of 18 years old who are having emotional or psychological difficulties as a result of their medical condition and who are inpatients or regularly attend the RHC.
The children we see are typically experiencing difficulties with their thoughts, feelings, behaviour and ability to cope, as a result of their medical condition, and this might be impacting their ability to manage their medical condition.
We also work with parents who require psychological intervention to help them adjust to their child’s condition or treatment in order that they can support their child as best they can.
There are lots of different reasons for a child or young person, with a diagnosed medical condition, and their family, to come to see a Clinical Psychologist. Children and young people who have been referred will be experiencing difficulties with their thoughts, feelings, behaviours and ability to cope. These difficulties will be as a result of their medical condition and/or will be impacting on their ability to manage their condition. Some of the most common reasons for referral are listed below.
Emotional Distress
Having a medical condition can sometimes make a child or young person feel anxious or scared, either about coming into hospital or about how to cope in daily life. Sometimes there are fears about the future, and how best to manage things. It often takes time to understand and accept a diagnosis or injury. Sometimes there will be feelings of anger, sadness and grief over the changes to life.
Adjustment
Sometimes children can become worried about their treatments, or just struggle to take their medication. It can take time and energy to stick to a medication regime. This can be harder still when it means time away from doing things that are fun or where you feel different or separate from your peers. Sometimes there are changes to how a child or young person looks or feels in their body, and adjustment to this can take time.
Acceptance
At other times it might be hard for a child and family to learn to accept and cope with living with a medical condition. Having a new diagnosis often means a big change to life for the whole family. There can be mixed feelings about these changes.
Trauma
Occasionally children and young people may be affected by traumatic events which have occurred at the time of diagnosis or injury or following complicated procedures. In the immediate aftermath of sudden scary events, distress and anxiety are normal responses. However, sometimes, after a longer period of time, the memory of these events can still trigger feelings of distress and can begin to interfere with day to day functioning.
Parental and Family Support
When a child or young person has become unwell or is given a new diagnosis, or where complex decisions must be made, parents can often benefit from the opportunity to reflect upon events and receive emotional support. We are also aware of the impact that a child with a medical condition can have on siblings within a family. Where possible we try to involve the whole family when offering support and advice.
Procedural Distress
The Play Specialists in the RHC do a lot to support children and young people with worries and understanding procedures but sometimes Clinical Psychology is needed too. Children or young people can often feel very anxious and distressed about having medical procedures, attending clinics or receiving feedback at clinics e.g. some young people with Diabetes feel really worried when attending clinics to discuss their HBA1C levels. This can often mean worry in the lead up to hospital appointments and finding it difficult to relax once they get here. Sometimes this can make them not want to come for procedures or attend clinics, or feel very upset when undergoing treatments.
Who We Are
Our team is made up of:
Clinical Psychologists
Child and Adolescent Therapists
Assistant Psychologists
Psychology Trainees
What Happens at an Appointment
Out-patient appointments with the Paediatric Clinical Psychology Service normally take place in the ‘Therapies Hub’ on the ground floor of the Children’s Hospital, also known as Clinic 12 or Clinic 1. If you are an in-patient, appointments will take place in a quiet room on the ward, or in a medical speciality clinic.
Assessment
First appointments will normally last between 45 minutes and an hour when we will meet with you and your parents/guardians. If you are a young person, we will give you the opportunity to meet on your own with the Clinical Psychologist for some of these appointments.
At a first appointment, it is helpful for us to hear all about you, your life, hobbies, school/college/work, friends and family, as well as the background of your medical condition. We will also think together about the difficulties that you have been experiencing, how these are impacting your life and condition, and how you and your family cope.
First appointments involve some talking and listening and sometimes drawing and playing with toys together too.
Follow-up
If it is thought that it would be helpful for you to return for further appointments, this will normally be arranged in the first appointment. Follow up appointments will allow us to get to know you better, formulate your difficulties and come up with a plan for supporting you and your family.
We use a number of different therapies, all of which have an evidence base. That is, we know from research that these can be helpful for children and young people struggling with the same kinds of difficulties as you. These might include, among others:
Cognitive Behavioural Therapy
Acceptance and Commitment Therapy
Solution Focused Therapy
Compassion Focused Therapy
Trauma-Focused Cognitive Behavioural Therapy
Family and Systemic Interventions
Motivational Interviewing Approaches
EMDR (Eye Movement Desensitisation and Response)
Narrative Therapy
Parenting Approaches
Guided Self Help
Group Approaches
Families may be seen on either an inpatient, outpatient basis or a combination of both.
Feedback, Complaints and Compliments
At the end of our work together, you will be asked to complete an Experience of Service questionnaire. The information you provide will be anonymous. This is an opportunity to let us know aspects of your care that you have found helpful or unhelpful.
We also welcome feedback via the Care Opinion website. For information about the NHS Greater Glasgow and Clyde complaints procedure, please visit our Complaints page.
What do Paediatric Psychology do to Help?
When we meet we will try to come to an understanding together of the things which are difficult for a child or young person and how best to help. We do this through talking and asking questions, but above all listening to what matters to that child or young person. We play games or draw together, to help us get to know a young person better. Sometimes we will ask a young person to keep a diary or chart to record their thoughts, feelings, actions or symptoms. For example – ‘My Emotions Worksheet’.
We use a number of different therapies, all of which have an evidence base. That is, we know from research that these can be helpful for children and young people struggling with the same kinds of difficulties as you. These might include, among others:
Cognitive Behavioural Therapy
Acceptance and Commitment Therapy
Solution Focused Therapy
Compassion Focused Therapy
Trauma Focused Cognitive Behavioural Therapy
Family and Systemic Interventions
Motivational lnterviewing Approaches
EMDR (Eye Movement Desensitisation and Response)
Guided Self Help
Group Work
In addition, we regularly run psycho-educational or therapeutic groups for parents or for young people. Both will have an opportunity to meet with and work with others with similar issues.
Teaching and Training
We contribute as a team to the teaching and training of other multi-disciplinary staff working with children within the hospital. We run regular CPD as part of the NHS Education Scotland Psychosocial Interventions Modules. We also teach students in training to become Clinical Psychologists and therefore have close links with the Doctoral courses at both the University of Glasgow and the University of Edinburgh.
Preparing for Hospital
Below are a number of websites, leaflets and links to other resources which can help you prepare your child for coming to hospital.
Preparing for Hospital – ‘What? Why? Children in Hospital’ Chartiy – This charity website gives access to videos and information to help you better support your child when coming into hospital.
The HospiChill App – The HospiChill App was designed by our Consultant Clinical Psychologist, Dr. Janie Donnan, and is downloadable from the apple apps website. It gives you options for saving upcoming appointments and lots of hints, tips and relaxation strategies which can be used through your phone, to help prepare you for coming into hospital.
The Hospital Passport – The Hospital Passport is a passport for children which can be brought in with them to each appointment. It includes space for preferences around treatment, stickers for achievements, and strategies for better coping. You can ask the pre-assessment team or your medical team for one of these if you think it would be helpful for your child.
RHC Specialist Play Service – We work closely with the Play Specialists, based in the Teddy Bear Hospital on the ground floor of the Children’s Hospital. This can be a helpful place for children to meet and work therapeutically with Play Specialists and familiarise themselves with the hospital environment through play with real and toy medical equipment. We or a child’s Consultant can make referrals to the Play Service on your behalf.
Having a Hospital Clinic Appointment (GOSH Information Sheets) – these are ‘easy to read’ information sheets from Great Ormond Street Hospital, London, for young children and children with learning disabilities, which explain what happens when you come for a hospital appointment. These include information on coming along for a CT scan, a blood test or an ECG, among others.
Resource for parents of children with ASD (Parents Guide to Blood Draws) – This resource has lots of good information and strategies on how best to prepare your child with Autistic Spectrum Disorder for having a blood test carried out, but could be applied to all young children.
Parents- Looking after Yourself
When times are difficult, it is really important for parents to take time out to look after themselves and their own mental health. Below are some resources which may be helpful.
We accept referrals from all medical specialities within the hospital. We have an embedded psychologist as part of the following Paediatric Medical Speciality Teams:
Burns (Supporting Children with Burns)
Cardiology
Diabetes
DSD (Differences in Sexual Development)
Feeding
Gastroenterology
OBPI (Obstetric Brachial Plexus Injury)
Oncology, Haematology and Stem Cell Transplant
Pain
Paediatric Intensive Care
Renal and Renal Transplant
Respiratory
Rheumatology
Links for Children and Young People
Below are some useful links and resources for children and young people.
HospiChill – downloadable app to help with worries related to hospital appointments, admissions and procedures
Paediatric Liaison Psychiatry Team
Welcome to the Paediatric Liaison Psychiatry Team at the Royal Hospital for Children (RHC). We are a specialist multi-disciplinary team offering mental health and neuropsychiatric assessments, interventions and consultations. We work on an inpatient and outpatient basis for children and young people who regularly attend medical or surgical teams at NHSGGC hospitals.
Who Are We?
Our multi-disciplinary team comprises of:
Child and Adolescent Psychiatrists
Clinical Psychologists
Mental Health Nurses
Family and Systemic Psychotherapist
* Medical, nursing and clinical psychology trainees are often part of the team.
Our Service
Our specialist team is available to children of all ages, all ranges of learning ability and from all geographical areas, as long as there is a clear role for the Paediatric Liaison Team.
Children and young people who are inpatients in a NHSGGC hospital are generally seen within one working day of referral. There is usually no waiting list for standard out-patient appointments.
We also provide an on-call service for advice and assessment regarding acute mental health presentations in children and adolescents within the RHC, and under-18s presenting to NHSGGC hospitals. We actively participate in research and audit to improve patient care.
How can we help?
We can offer a number of services:
On call assessment for acute mental health presentations Monday to Friday 9am – 5pm.
Routine assessment and treatment of mental health difficulties in children and adolescents who are frequent attenders of Paediatrics within RHC.
Advice, if needed urgently, regarding the mental health of a parent or care giver of a young person who is an inpatient.
Joint working with other hospital-based professionals, such as:
Supporting paediatric staff with care planning and management of admissions for young people with learning disabilities, neurodevelopmental disorders or complex mental health difficulties, who require psychologically informed approaches to their care.
Liaison with Paediatric Clinical Psychology and Child and Adolescent Mental Health Services (CAMHS), education and social work.
Consultation to other hospital based and community services.
Training to paediatric staff regarding mental health and neurodevelopment and neuropsychiatric conditions.
The Way We Work
We offer an initial assessment to determine what service would be most helpful. Where possible the child or young person and their family are assessed initially by two members of the team. We frequently find it useful to work together with paediatric colleagues to complete an assessment.
Following assessment, we may discuss referral to another service that would be more appropriate to meet the child and family’s needs. If our service is the most appropriate we may offer individual work, family work and/or medication advice as deemed appropriate. In some cases we may refer the case on to a more appropriate service.
The team uses a range of therapies including:
Cognitive Behavioural Therapy
Compassion Focussed Therapy
Acceptance and Commitment Therapy
Family and Systemic Interventions
Problem Solving Approaches
Families may be seen on either an inpatient or outpatient basis or a combination of both.
Reasons for Referral
Referrals are accepted where there are complex mental health needs. Our referral criteria is as follows:
The child/young person should be under 18 years of age and under the care of a Consultant at the RHC, Glasgow Royal Infirmary, Queen Elizabeth University Hospital, Royal Alexandra Hospital or Inverclyde Royal Hospital and
Require acute mental health assessment or
Have a physical health condition/symptoms or neuropsychiatric condition that is causing significant psychological/behavioural or mental health difficulty (this includes medically unexplained or functional symptoms, complex pain disorders and chronic fatigue syndromes requiring regular outpatient or inpatient care at the RHC) or
Have a significant psychological/behavioural/mental health difficulty which is directly impacting on their ability to engage with treatment, posing a significant or immediate risk to the child/young person or
Have an existing learning disability, neurodevelopmental condition or neuropsychiatric or mental health diagnosis and require support to manage admission or treatment at the RHC.
How do I make a Referral?
We accept referrals from hospital consultants, nurse specialists, allied health professionals and locality CAMHS. All referrals should be directed to the Paediatric Liaison Psychiatry Business Support Team in the first instance – 0141 451 6529 (86529 for internal calls).
What if it’s Urgent?
It is expected that urgent referrals will be made via telephone contact. The team offers an on-call service Monday to Friday from 9am to 5pm. If an urgent psychiatric response is specifically required and cannot be achieved within team working hours, the referral is passed to the Out of Hour’s duty clinician available via the RHC switchboard (0141 201 0000).
When making an urgent referral, please provide the following information:
Patient’s full name
CHI/DOB
Ward/location
Named consultant
Reason for admission
Mental health concerns
Urgent referrals are seen within 24 hours
What if it’s Non-Urgent?
For non-urgent referrals, we require that referrers provide the following essential written details:
Patient’s full name
CHI/DOB
Ward if an inpatient
Named consultant
Reason for referral
Aims of referral
The Paediatric Liaison Psychiatry Business Support Team will provide a referral pro-forma for completion to action referral. The team meets weekly on Wednesday mornings to review new referrals and allocate where appropriate.
Out of Hours Services
Out with the Paediatric Liaison Psychiatry working hours, Monday-Friday 9am – 5pm, emergency referrals should be directed to the Out of Hours duty clinician, accessed by phoning the RHC switchboard on 0141 201 0000 (1000 for internal calls).
Alternative Services – Community and Hospital Based
The Paediatric Liaison Psychiatry team is one of a number of services available to meet the emotional and behavioural needs of children, young people and families. Other services include:
Services based at the Royal Hospital for Children:
Paediatric Clinical Psychology
Paediatric Neuropsychology
Family Bereavement Service
Family Support and Information Service
Chaplaincy and Spiritual Care
Community Based Services
Child and Adolescent Mental Health Teams (CAMHS) including ICAMHS
If there is uncertainty about which service is most suitable for a referral, this can be discussed with our on-call clinician, who is responsible for taking referrals that day. Referrals that require psychological input based within RHC, but not the expertise of a multi-disciplinary mental health team, may be discussed with the Paediatric Clinical Psychology Service.
If RHC based input is not required, but there is a mental health need, referrals may be passed to an appropriate community team or specialist service after discussion with the referrer, or guidance may be given on services and resources.
Contact Paediatric Liaison Psychiatry
You can contact the Paediatric Liaison Psychiatry Team at:
Paediatric Liaison Psychiatry Team Business Support Office Block, Zone 2.01 Royal Hospital for Children Queen Elizabeth University Hospital 1345 Govan Road Glasgow G51 4TF
If you are in a ward in the hospital you can ask one of the nurses to call us using the number above.
Paediatric Neuropsychology Service
The Paediatric Neuropsychology Service (PNS) is a small team of Clinical Psychologists, based at the Royal Hospital for Children, Glasgow. We see children and young people aged 0-18 years, who attend RHC because of a condition that originates in their central nervous system and affects their functioning. This includes children with epilepsy, brain tumours, infections, strokes and head trauma.
We accept both inpatient and outpatient referrals; most of our referrals come from neurology, neurosurgery and neuro-oncology.
Our main job is to assess children’s cognitive, behavioural and emotional functioning and make sense of these in the context of their neurological/developmental condition.
Most children and young people will have a standardised cognitive assessment as part of their contact with the service. This involves them completing a series of puzzles which are designed to find out their cognitive strengths and weaknesses.
We then make recommendations about how they can best be supported at home, school and in their community.
Enquires can be made to
Paediatric Neuropsychology Service Office Block, Zone 2.01 Royal Hospital for Children Queen Elizabeth University Hospital 1345 Govan Road Glasgow G51 4TF
All children and young people who require it should access Child and Adolescent Mental Health Services (CAMHS) at the team local to where they live. Within CAMHS services there are additional supports for children and young people who have a learning disability, whose experiences of adversity past and present have resulted in complex trauma, or who have forensic mental health needs. This supports CAMHS teams in working with these vulnerable groups of children and enables equitable access to mental health services for these children and young people.
The Tier 4 Hub is a specialist service that works with children and young people (0-18 years) at greatest risk and who require a period of intensive assessment and intervention and/or specialist intervention. We work with children and young people with mental health disorders and who have
Learning disabilities and/or
Experience of complex trauma and/or
Severe conduct or offending behaviour (Forensic).
The Tier 4 Hub become involved at the request of their colleagues in the locality of CAMHS.
We are based at
Floor 1 Building 3 Templeton Business Centre 62 Templeton Street Glasgow G40 1DA Telephone 0141 201 0808
Learning Disabilities
Young people with a learning disability may have difficulties in understanding situations, in expressing themselves, or have fewer opportunities to learn about becoming older and more independent. They can have the same mental health problems as other young people who do not have learning disabilities, but these might look different, be more difficult to detect, and need interventions and treatments that are adjusted to suit individual needs.
Children and young people with learning disabilities, and their families and carers, can expect CAMHS to make reasonable adjustments to enable them to be helped by CAMHS. This might be having an appointment at home rather than in a clinic, having a longer appointment time, using playing and drawing instead of talking, working with parents and carers and others instead of directly with the child, joining with the family, school, health services provided through the school, social work services, etc. in reviews or discussions to think together about the difficulties and how best to help.
The learning disability clinicians in CAMHS are experienced in working with children and young people and with people with learning disabilities and can help with ideas and suggestions about how to understand and tackle problems. This might be working directly with families and other agencies, or supporting their CAMHS colleagues to work with children and young people affected by learning disability.
Some learning disabilities clinicians are based in the local CAMHS teams and others in the ‘Tier 4 HUB’. They are a multi-disciplinary team with skills in learning disability child and adolescent mental health and challenging behaviour (Consultant Child and Adolescent & Learning Disability Psychiatry; Registered Learning Disability Nursing; Clinical Psychology; Speech and Language Therapy; Occupational Therapy; Clinical Support Worker).
Complex Trauma
‘Trauma’ is a widely used term, but in this context it refers to: an event which is exceptionally threatening or catastrophic and is likely to cause distress for almost everyone.
Complex trauma is when these traumatic events are repeated and interpersonal (inflicted by other people). This includes childhood sexual abuse, childhood physical abuse, witnessing domestic abuse, war and neglect. Please note this is not an exhaustive list.
Children and young people with a complex trauma history can develop mental health difficulties which may lead to them presenting in CAMHS.
The Complex Trauma Pathway aims to support our colleagues in the locality CAMHS teams to provide a trauma sensitive approach to their input with young people who have a complex trauma history. As well as provide specialist input directly to young people and their families where needed.
You can find out more about the Complex Trauma Pathway by watching the video.
Forensic Child and Adolescent Mental Health Services (FCAMHS)
Information for Young People
What is FCAMHS?
We work with young people who are going through a hard time. You might be getting into trouble with the police and having problems with your mental health.
We have a psychiatrist, speech and language therapist, occupational therapist, psychotherapists and psychologists on our team.
Who comes to FCAMHS?
We see young people under the age of 18. Some have been charged with a serious offence. Some are involved with the police or youth justice social work. Some are in secure care.
What can I expect if I see FCAMHS?
You might already be coming to CAMHS. If you are, your CAMHS worker will introduce us. We can see you at your local CAMHS team. Sometimes we might see you somewhere else e.g. if you are in secure care. When we meet we will tell you about our service. We will also want to find out more about you. We want to listen to you. Then we decide together if we are the best team for you.
What happens when I come to FCAMHS?
We listen to you and talk about the problems you are having. We work with you to understand why you are getting into trouble. We speak with people who know you well. We want to understand how to keep you and other people safe. We work with teachers, social workers and secure care staff to help us think about the best way to keeping you safe and out of trouble.
What else might happen?
We will ask you to fill out a form when we first meet. You might also have to fill out a form at the end. We do this to see if our team is working well. We might ask you what you thought of working with us. We want to know how we can improve.
How can I get help from FCAMHS?
If you are being seen by CAMHS your worker might ask FCAMHS to see you. If you are in secure care then your GP or Social Worker might ask FCAMHS to see you. If you go to ISMS (Glasgow City Council’s Intensive Support and Monitoring Service), then your ISMS worker will ask you to meet with FCAMHS.
Information for Professionals
Who are we?
FCAMHS was developed following a review of the needs of young people who are involved in serious offending behaviour across Greater Glasgow and Clyde (GG&C). We now sit as part of the Tier 4 CAMHS hub, alongside work-streams for complex trauma, and intellectual disability.
The service is a multi-disciplinary team, consisting of Psychology, Psychiatry and a Social Worker. We also have access to Speech and Language Therapy, Occupational Therapy, and Psychotherapy. Unlike the other work-streams, FCAMHS do not have link-nurses. We have therefore, been working to establish links with Tier 3 teams across GG&C.
FCAMHS also consists of commissioned services who offer direct access to children in Secure Care, or children accessing the Glasgow City Council Intensive Support and Monitoring Service (ISMS)
Who is the service for?
We offer a provision for young people up to age 18 living within the GG&C area who have moderate to severe mental health difficulties, and who present a significant risk of harm to others by means of physical or sexual violence or fire-setting. Typically, these are complex cases requiring intensive MDT working and assertive outreach, that may outstrip Tier 3 resources.
What do we do?
We can provide specialist assessment of risk, using structured professional judgement approaches, which are evidenced-based and recommended by the Risk Management Authority.
We support those working with young people to understand the development and maintenance of offending behaviour. This subsequently underpins a holistic ‘Whole Systems’ intervention and care plan to reduce risk.
We can provide assessment and intervention for serious and chronic mental disorder, particularly when this is associated with risk. We also offer interventions focussing on reducing offending.
We support colleagues in Tier 3 CAMHS, by providing specialist training in relation to forensic issues.
We routinely evaluate our services, as well as developing clinical research projects.
How to request assistance.
Requests for assistance come from locality CAMHS teams. All requests are addressed to the Tier 4 Hub. In order to do this, you can contact the FCAMHS duty clinician to discuss. We will request initial assessment and risk (FACE CARAS) reports. We will discuss within weekly Tier 4 referral meeting and the case will be allocated if accepted.
If you are referring for a child not known to GG&C CAMHS, but who is residing in Secure Care, then a referral form can be requested from the unit and sent to: F.CAMHS@ggc.scot.nhs.uk
All referrals from secure care should be discussed with the child, their consent sought and also sent to the above email address. Both referral and consent forms can be obtained from the secure units.
Unscheduled CAMHS (UCAMHS)
Unscheduled Child and Adolescent Mental Health Services (UCAMHS) is a specially trained team of CAMHS Nurses and Health Care Support Workers. We support children and young people who are experiencing significant distress and/or mental health difficulties.
What do we do?
We are part of an urgent response pathway which responds to children and young people’s urgent mental health difficulties. We offer support 24 hours a day, 7 days a week. We can offer:
support and advice to front line services,
assessment and treatment for urgent mental health issues,
access to inpatient medical and psychiatric care.
When a young person is referred to UCAMHS, we will:
speak with the referrer to gather information and decide whether an urgent mental health assessment is needed and what kind of assessment would best support the young person
offer support/advice over the telephone
when appropriate arrange a telephone and/or face-to-face appointment to understand the young person’s mental state and identify any care needs
carry out safety planning to help manage any risks
work together with the young person, their family and other professionals and agencies
make sure the young person gets the right support by making referrals to other appropriate services.
If a face to face assessment is required someone from the UCAMHS Team will visit the young person in any NHSGGC hospital. Young people aged 16-17, who don’t need medical treatment, might be seen in the Mental Health Assessment Unit.
How do you make a referral?
Referrals to UCAMHS can be made by telephone by:
NHSGGC paediatric and adult general hospital wards and Emergency Departments
Out of Hours GP
NHSGGC CAMHS
Police
Scottish Ambulance Service (SAS)
Tier 3 Locality CAMHS
Who is UCAMHS for?
UCAMHS can support young people who are:
Under 18 years of age
Not currently open to the Esteem Team
Present within NHSGGC at time of referral
Experiencing significant distress and/or mental health concern requiring urgent specialised mental health care.
Specialist Community Paediatric Teams
Specialist Community Paediatric (SCP) Teams work with babies, children and young people with a variety of disabilities and genetic conditions and those who are developing differently to what would be expected. They work in the community to support those who have ongoing needs but don’t need to be in hospital. They work to identify, assess, diagnosis, treat, support and monitor babies, children and young people.
SCP Teams are made up of different health professionals including Nurses, Occupational Therapists, Paediatricians, Physiotherapists, and Speech and Language Therapists. Children and young people might be seen by one or more of these professionals together or separately depending on what they need. The SCP Teams work with the baby/child/young person, their family and the team around them (such as Education, Social Work, Third Sector professionals). How they work will change over time depending on what the baby, child or young person needs.
There are 6 teams based in Children’s Centres across NHS Greater Glasgow and Clyde (GGC). The professionals who make up these teams work together or separately to support children and young people to reach their potential. You can find out more about our SCP Teams and the professionals who make up these teams on KIDS for Families.
Nursing
There are 4 different nursing teams working within 4 pathways of care in the community. These teams are the:
Additional Support for Learning (ASL) Nurses (including Mainstream Nurse Trainers)
The Additional Support for Learning (ASL) Nursing Teams all align to the Health and Social Care Partnerships (HSCPs). They work in the geographical areas and teams. In Glasgow, there are 11 ASL schools. There are 3 ASL schools in the Clyde areas. These schools are attended by children with various complex needs/physical impairments/visual impairments and learning disabilities.
The ASL Nursing Team provide training, advice and support to Education staff to enable children and young people with complex needs to access their education. They also carry out the school-aged immunisation schedule within the ASL schools. The team carry out Nurse-Led Assessments offering a holistic overview of health and social needs. They offer support, advice, training, referral and signposting as appropriate. This is in collaboration with the Community Paediatricians who assess children at specific points in the child’s school career and may see the more complex children and young people if appropriate. The team provide support packages for sleep difficulties and develop individual sleep programmes. The team also carry out regular health screening such as height, weight and Thyroid Stimulating Hormone (TSH) screening for children and young people with Down’s Syndrome.
The ASL Mainstream Nurse Training (MNT) team also provide training, advice and support for Nurseries/Family Centres, Mainstream Schools and Moderate Learning Difficulties (MLD) schools. They also carry out Nurse-Led Assessments where beneficial to the child and family.
Referrals to the MNT team are received from various routes including:
Education
Specialist Nurses at the Royal Hospital for Children (RHC)
The Community Children Nurses across NHS Greater Glasgow and Clyde (NHSGGC) area support children and young people aged 0-18 years. They support healthcare within the home/community setting where a need has been identified.
They support services across NHSGGC locations for acute and short term conditions;
Children with long-term/chronic conditions who require treatment monitoring, advice and support.
Children with complex needs and exceptional complex care needs who require continuing care.
Children with life-limiting and life-threatening illnesses, including palliative and end-of-life care.
Transitions into adult care.
The team provide individual, person-centred holistic nursing incorporating; assessment; treatment; monitoring; advice and support and education and training. The staff work in partnership with parents and carers and a wide range of professionals that work around the child. The initial home visit will be by a qualified nurse who will carry out a holistic assessment and then plan ongoing risk and health care needs.
Referrals to the service are received from a hospital letter, clinics, discharge letters, EMIS referrals, email, post and telephone. They come from a number of sources, such as:
Acute and community services
Primary health care
Allied health professionals
Parents/Carers
Specialist nurses
Education services
Professionals out with NHS GGC board area
Other specialist children services
CCN Services Locations
Glasgow
Floor 1 Building 3 Templeton Business Centre 62 Templeton Street Glasgow G40 1DA
Inverclyde
Skylark Centre L-North Inverclyde Royal Hospital Larkfield Road Greenock PA16 0XN
Aranthrue Centre 103 Paisley Road Renfrew Renfrewshire PA4 8LH
West Dunbartonshire
Acorn Centre Vale of Leven Hospital Main Street Alexandria West Dunbartonshire G83 0UA
Disability Nurses
The Disability Nurses work as part of the specialist community paediatric teams across Greater Glasgow and Clyde. They are located across the 7 child development centres.
They support newly identified children and young people with neuro-disability or developmental concerns and suspected neurodevelopmental conditions. They use a holistic person-centred approach to complete an initial assessment. A full developmental history and background is taken to identify concerns and future needs. This helps to identify which professionals need to be involved in the child’s care.
The team then supports robust assessment, diagnosis, advice, onward signposting and referral. They also advocate for the child or young person. They support ongoing reviews and interventions.
The team also support ongoing care and reviews for children with complex disability. The nurses work closely with paediatricians and AHPs to support the provision for children and their families. They do this by having a strong understanding of the needs of the local area.
They may take on the health lead professional role to support vulnerable and complex children with neuro-disabilities, developmental disorders, long-term conditions and physical disabilities. They also work closely with social work colleagues to support those who are care experienced and at risk.
Referrals come from a range of professionals including:
Health Visitors
School Nurses
GPs
Neonatal and Hospital Professionals
Education Professionals
Social work
The Disability Nurses report to referrers and GPs via standardised reports to ensure appropriate communication. These reports are also shared with parents/carers.
Disability Nurses Services Locations
Glasgow
Bridgeton Child Centre 201 Abercromby Street Glasgow G40 2DA Tel: 0141 531 6550
New Gorbals Health and Care Centre 2 Sandiefield Road Glasgow G5 9AB Tel: 0141 201 5000
West Centre 60 Kinfauns Drive Glasgow G15 7TS Tel: 0141 207 7100
Woodside Health and Care Centre 891 Garscube Road Glasgow G20 7ER Tel: 0141 201 5665
Inverclyde
Skylark Centre L-North Inverclyde Royal Hospital Larkfield Road Greenock PA16 0XN
Health for All Team (Care Experienced Children and Young People
This unique nursing and medical service supports the holistic health assessment of care experienced children and young people. The children and young people may live in kinship care, foster care, residential units or specialist units. The team also support unaccompanied minors, and asylum-seeking young people. The team aims to improve health outcomes for these children and young people. They use standardised assessment tools and early interventions. They also use a GIRFEC approach and a trauma-informed approach. Using these approaches they support #the promise, to ensure the best possible care and collaboration for care-experienced children and young people.
Referrals come from Social Work Services. There is close communication and joint planning for this population.
The services are delivered from 4 locations in NHSGGC.
Glasgow
Health for All Team Specialist Children’s Services Floor 4, Building 2, Templeton on the Green 62 Templeton Street Glasgow G40 1DA
Inverclyde
Health for All Team Specialist Children’s Services L-North Inverclyde Royal Hospital Larkfield Road Greenock PA16 0XN
Renfrewshire
Health for All Team Specialist Children’s Services Aranthrue Centre 103 Paisley Road Renfrew Renfrewshire PA4 8LH
West Dunbartonshire
Health for All Team Specialist Children’s Services Suite 3rd floor Maternity Building Vale of Leven Hospital Main Street Alexandria G83 0UA
Occupational Therapy
Occupational Therapists can support you to join in (participate in) every day activities (occupations) to help you lead a full and happy life, reach your goals and learn the skills you will need during your life to be an active member of your community.
We aim to support you to do the things that you want and need to do. We do this by thinking about you, the occupation and the environment. If these three things are not working together then it can be hard to take part. We can help you to make changes to improve your enjoyment in everyday life.
Community paediatricians are specialist doctors who provide out of hospital care for children and young people with long term disabilities with a focus on their participation and quality of life.
The role of the community paediatrician involves identification, assessment, diagnosis, treatment and support of children and young people with long term neuro-disability (such as Cerebral Palsy), genetic conditions (such as Downs Syndrome) and those with specific neuro-developmental conditions. Community paediatricians have a key role in co-ordinating the team around child and young person by working closely with multiple agencies including Health (hospital clinicians and allied health professionals), Education and Social Care.
Children’s Physiotherapy is the management and care of babies, children and young people from birth to 18 years or school leaving age (some young people may be directed to adult services as appropriate).
Physiotherapists work together with children, young people, their families and others involved in their care. They support children and young people to reach their physical potential.
The Physiotherapy Team is made up of Physiotherapists and Physiotherapy Clinical Support Workers. If needed, the child/young person will be allocated to a named Physiotherapist. This Physiotherapist will help to support you and your child/young person. They will work alongside the team around your child/young person.
Children and young people can have speech, language and communication issues. These issues can stop them from joining in with others and participating in daily life. Some children do not understand what is being said to them or struggle to put words together. A child’s speech may be hard to understand or they may find interaction difficult. Children with communication difficulties may need Speech and Language Therapy.
Speech and Language Therapists assess and support children and young people with communication and/or eating and drinking difficulties.
Sometimes a child’s communication difficulties can have an impact on their everyday life. The Speech and Language Therapy team can offer advice and information to families, nurseries and schools. We will always give advice and ideas on how to support children and young people in their everyday life.
This page provides information about our Healthy Minds mental health awareness-raising resource. If you have any questions about the resource or would like to hear more about it, please contact ggc.mhead@nhs.scot.
*Please note that this is a generic admin inbox and not monitored immediately. If you, or someone you know are in distress and need an immediate response call the emergency services on 999 or NHS24 on 111.
What is the Healthy Minds resource?
Healthy Minds is a universal resource which aims to promote basic awareness and understanding of mental health and topics that are associated with and can impact on mental health and wellbeing. It is a cascading and capacity building resource that aims to support partners and organisations deliver on the public mental health agenda. The focus of Healthy Minds is prevention and early intervention.
The sessions can be delivered in person or online. Please read our Healthy Minds information leaflet carefully before accessing the resource: Healthy Minds Information leaflet.
Who can use Healthy Minds?
The resource is aimed at anyone who has an interest in raising awareness of mental health and wellbeing. You don’t need any prior experience or qualifications to deliver any of the sessions. It is not a training resource but a tool to raise awareness of basic mental health and areas that can impact on mental health and wellbeing.
Healthy Minds by NHS Greater Glasgow and Clyde is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, meaning it can be used and adapted to suit your own purposes.
The Healthy Minds Collection
There are 20 sessions available to download on a range of areas that can impact mental health and wellbeing. Each session has a PowerPoint presentation, facilitator’s notes, and handout to guide you through delivering the sessions.
Translations to Arabic, Mandarin, Polish, Romanian, or Urdu are available for some sessions, including Basic Mental Health Awareness (01) and Menopause (17).
You can browse the full collection below:
00. Healthy Minds Information Session
Anyone can deliver a Healthy Minds session to raise awareness of mental health and the factors that can impact it. To help you deliver these sessions with your staff, team, or partners, we have developed a dedicated Healthy Minds Information Session. This introductory session gives an overview of the resource, including what it is, why it was developed, and how to access it.
Included as part of this are a PowerPoint presentation, facilitator’s notes, and a frequently asked questions document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
For those who are looking to deliver the Healthy Minds sessions online using a virtual learning space such as Microsoft Teams or Zoom, we have also developed an online guidance document:
The Mental Health Improvement team are a Greater Glasgow and Clyde wide team who support our colleagues and partners across the six Health and Social Care Partnership areas with public mental health; Glasgow City, Renfrewshire, East Renfrewshire, West Dunbartonshire, East Dunbartonshire, and Inverclyde.
We share updates about the work we are undertaking across our key priority areas, and share useful resources and information to help you deliver on the public mental health agenda.
This is not a website for people looking for immediate help. If you are in distress and need immediate help:
Please contact the Central Booking Office on 0141 347 8406
The Central Booking Office is open
Monday to Friday: 9:00am – 4:00pm
Saturday: closed
Sunday: closed
There is no provision for childcare during your MRI scan. If you need to bring a child, please ensure there is also a responsible adult to look after them or we may not be able to perform your scan.
Department Opening Hours
Monday – Friday: 8:45am to 5:00pm
Department Location
Glasgow Royal Infirmary 84 Castle Street Glasgow G4 0SF
We use cookies to analyse traffic to our site and to enable certain functions such as forms and YouTube videos. These do not collect personal information. By clicking "Accept All", you consent to our use of cookies, or you can customise the options.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
CloudFlare provides web performance and security solutions, enhancing site speed and protecting against threats.
Sequence rules uses cookies to track the order of requests a user has made and the time between requests and makes them available via Cloudflare Rules. This allows you to write rules that match valid or invalid sequences. The specific cookies used to validate sequences are called sequence cookies.
session
cf_ob_info
The cf_ob_info cookie provides information on: The HTTP Status Code returned by the origin web server. The Ray ID of the original failed request. The data center serving the traffic
session
cf_chl_rc_m
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
__cfruid
Used by the content network, Cloudflare, to identify trusted web traffic.
session
__cf_bm
Cloudflare's bot products identify and mitigate automated traffic to protect your site from bad bots. Cloudflare places the __cf_bm cookie on End User devices that access Customer sites that are protected by Bot Management or Bot Fight Mode. The __cf_bm cookie is necessary for the proper functioning of these bot solutions.
session
__cflb
When enabling session affinity with Cloudflare Load Balancer, Cloudflare sets a __cflb cookie with a unique value on the first response to the requesting client. Cloudflare routes future requests to the same origin, optimizing network resource usage. In the event of a failover, Cloudflare sets a new __cflb cookie to direct future requests to the failover pool.
session
_cfuvid
The _cfuvid cookie is only set when a site uses this option in a Rate Limiting Rule, and is only used to allow the Cloudflare WAF to distinguish individual users who share the same IP address.
session
cf_clearance
Whether a CAPTCHA or Javascript challenge has been solved.
session
cf_use_ob
The cf_use_ob cookie informs Cloudflare to fetch the requested resource from the Always Online cache on the designated port. Applicable values are: 0, 80, and 443. The cf_ob_info and cf_use_ob cookies are persistent cookies that expire after 30 seconds.
session
__cfwaitingroom
The __cfwaitingroom cookie is only used to track visitors that access a waiting room enabled host and path combination for a zone. Visitors using a browser that does not accept cookies cannot visit the host and path combination while the waiting room is active.
session
cf_chl_rc_i
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
cf_chl_rc_ni
These cookies are for internal use which allows Cloudflare to identify production issues on clients.